COVID UPDATE – H&R2020 Postponed!
So final decision was taken a few days ago to postpone H&R2020, for several reasons, mainly to be consistent in limiting large groups of humans in a room, but also fully understanding that the attendance of many faculty and participants is already in doubt, and we do not want to put forth a sub-par educational event. We are targeting september, tentatively 23rd to 25th, to be confirmed.
The options are the following:
We will (a) issue full refunds or (b) hold your spot for september. Each participant should please let us know which works best for you by emailing hospresusconference@gmail.com.
Please follow this page for further developments.
The H&R Team
We’re really excited for the third edition of H&R!
Last year was great, all thanks going to our awesome faculty, and this year, we’re planning on taking it yet to another level. We’ve added some new faculty members who’ll be bringing some interesting perspectives, and there will be a pervasive theme across the two days to really get everyone’s understanding and management of the oft-overlooked venous/right side of things, woven in among the other key topics that last year’s attendees and the scientific committee chose. This is a clear evolution in clinical practice that, paired with POCUS, is really a game changer across a wide range of pathologies. Expect to leave from these two days with at least one extra notch on your belt.
The importance of careful fluid resuscitation has been gaining attention in the last years – take for instance the great work being done by Manu Malbrain at IFAD (International Fluid Academy) who just had their symposium. Treating fluids like the drugs that they are should be our goal.
In addition we have picked a number of important topics, with the idea to share knowledge and practical skills at therapeutic decision points, or else to bring attention to bleeding-edge topics that, though not widespread today, hold promise for further fine-tuning of resuscitation. One in particular is the use of the pulmonary artery catheter, whose use, though having fallen out of mainstream favour, persisted in many areas where clinicians were able to properly use this powerful monitoring tool. We feel it is poised to make a comeback among high-level resuscitationists. For some, it may be a matter of refreshing and re-polishing, and for the new generation, a good time to learn.
PRE-CONFERENCE COURSES!
There’s 4 of them, all on May 20th:
- The Hospitalist Course (full day)
- The Resuscitationist’s Toolbox (half day AM)
- Resus TEE (full day)
- Jiu-Jitsu for MDs (half day PM)
So, some slight structural adjustments. The Hospitalist angle now gets a pre-conference course, focusing on very practical, applied and critically important topics for the ward patients, including solid POCUS workshops to get some hands-on work on and great participant to faculty ratios. For the full programme of The Hospitalist Course see here.

We will do a Resuscitationists’ Toolbox pre-conference in which to learn or practice certain key skills for the high-level resuscitationist, such as REBOA, the PA catheter, surgical airways and more.

Felipe Teran and his team will bring back Resuscitative TEE, and registration is opening Thursday December 12th! There are only 24 spots, and until march 1st, priority will be given to H&R2020 registrants. Participants must first register for H&R2020, then email hospresusconference@gmail.com and indicate they want to attend the TEE course, following which a unique code will be provided which will be necessary for course registration at resusicativetee. After March 1st, remaining spots will be released for non-conference attendees. (HINT – last year, the course sold out in 5 days!!!)
Here is how to register after having obtained the code:
And yes, the Jiu-Jitsu workshop is back by popular demand!
THE MAIN EVENT!
The two main conference days will be packed full of interesting talks, both by traditional but exceptional academics, as well as many of the top notch #FOAMed educators. The tail end will have some awesome workshops for those who want to add to their skill set.
And, on a first-come, first-served basis, Early Bird Registrants will be able to book some one-on-one time with faculty – The Personal Workshop – for hands-on or discussion or skills workshop. To do so, register for the free early bird workshop and email hospresusconference@gmail.com to indicate your choice of instructor and topic!
Organized by The Critical Care & Ultrasound Institute for the Santa Cabrini Intensive Care Service at the CIUSSS E-MTL.
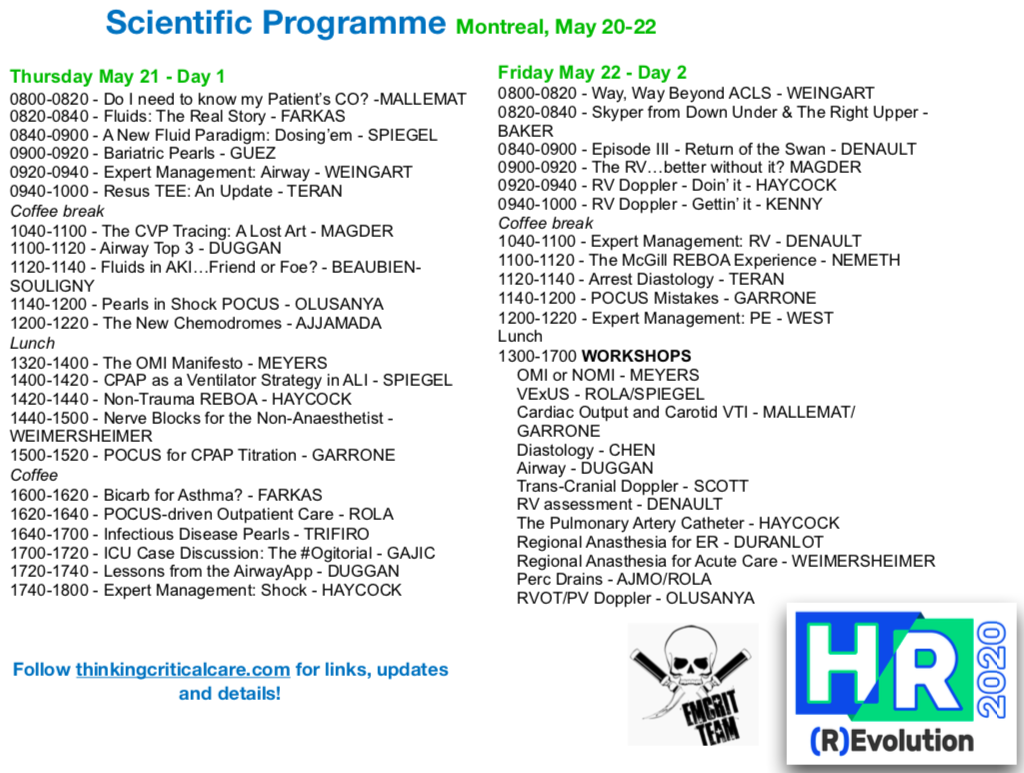
So here is the programme:


and in pdf: H&R 2020 Poster
All of this will be in Montreal, Quebec, Canada, most probably Santa Cabrini Hospital, but full details to follow!
Follow the blog and bookmark this page for conference updates!
The lineup so far… and more to come!

See you there!

Click Here to register!
Scientific Committee
Dr. Carol Zambrana
Dr. Philippe St-Arnaud
Dr. Joe Nemeth
Dr. Quoc Huy Ton-That
Dr. Mario Rizzi
Dr. Philippe Rola