
This, in my opinion, is an under-recognized problem when bedside ultrasound is NOT a routine part of examination of critically ill patients. I’m happy to say that as many of my colleagues have been picking up probes, it is somewhat less of an issue now, whereas a couple of years ago I’d often put in 4 or 5 pigtail catheters on day 1 of taking over the ICU.
The first and foremost reason for this is that the portable supine ICU CXR sucks at picking up the small to moderate to, yes, even the large pleural effusion. Largely owing to the fact that many of our patients have some lung parenchymal abnormalities and to the recumbent position that causes a layering of the effusion, it is often difficult to properly assess the size of a pleural effusion. Radiologists will usually report the presence of a probable effusion, but quantification is difficult, and physicians not performing routing bedside sonography will often realize the presence of a submassive effusion only on CT scan – after all it isn’t like you can turn and rotate your patient to percuss the shifting dullness, can you? Not very practical.
So the following can often be seen:
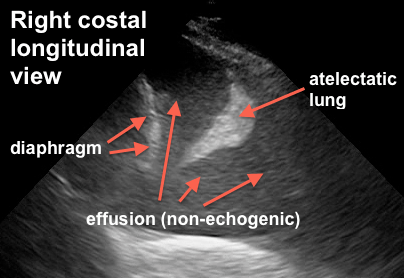
this is fairly large, or you might see:

So the obvious and critical question is: when is it necessary to drain?
There are two elements to this question:
a) for diagnostic purposes: unless the diagnosis is clear (eg CHF, post-resuscitation “michelin man” patient, etc) a new effusion should be tapped. Panapneumonic effusions, in particular, warrant ruling out empyema unless there is a compelling reason not to. For diagnostic purposes a 22g needle usually does the trick unless you have frank pus – which generally shows up differently on ultrasound.
b) for therapeutic purposes: effusions are space occupying lesions which compress the lung and result in a variable degree of respiratory compromise, depending on chest wall and diaphragmatic compliance, as well as effusion volume. The clinical effect is highly variable due to the above as well as the degree of parenchymal lung disease and the degree of PEEP. In the ICU or ED, a simple way to think about it is that if your patient is in respiratory failure and has a large effusion, chances are that draining it will improve things. It gets a little more controversial and complicated if you have a patient who is mildly dyspneic with a moderate sized effusion.
Here are a few clinical scenarios I like:
Mr. A is a 65 year old man with CHF, intubated, with large bilateral effusions. He has been aggressively diuresed to the point of his IVC being less than 5mm in diameter. He has not been able to wean in the last 48 h.
Yes, I definitely drain this fellow. Been there and done that time and time again. The pleural effusions are essentially the last to resolve (being the most “distal” to the circulation – vs the alveolar tissue itself) and hence can lag and cost a few more days or more of ventilation).
Mr. B is a 47 year old man with pneumonia, breathing spontaneously with a moderate (maybe 500ml) effusion. It appears free flowing and clear, he is afebrile with an improving white count, and mildly dyspneic.
Nah, I skip on this one. If fever and WBC recur, I do a diagnostic tap to r/o empyema.
Mrs. C is intubated on PEEP 18 FiO2 85% for ARDS due to pancreatitis. She has some degree of intraabdominal hypertension (IAP 18) and has bilateral moderate pleural effusions, maybe 400-500ml.
Yup. She can physiologically benefit from decreased intra-thoracic pressure, both from the ventilatory and the intra-abdominal pressure standpoint (Remember the diaphragm is not a rigid structure so that IAP and ITP are very similar in most cases).
So is there any evidence for this? Some. And that’s for part 2, coming within the next days. Part three will explain and show my procedure of choice for drainage.
Thanks!
love to hear what other guys’ practices are! Apparently only about 15% of ICU guys “routinely” drain effusions.
Philippe
COMMENTS
Hi Philippe,
I am very happy to read your post tonight, bacause I am part of that 15% and luckily most of my colleagues are in the same group. I agree in particular when you say that pleural effusions are the last to resolve, being the most “distal” to the circulation. I often find patients, at a certain point during their ICU stay, be not only like a “michelin man” but also (and at the same time!) hypovolemic. I call this situation, when I try to explain it to residents, “empty in full” (maybe in english it doesn’t sound as good as in italian): we are trying with diuretics and some fluid restriction to manage those extravascular fluids that prevent weaning from mechanical ventilation, but often we get the only effect of causing renal failure rather than eliminating pleural effusions. In this case the only way is to drain.
Another important point is that bedside chest x-ray is absolutely useless when you have to discriminate between pleural effusion and parenchimal consolidation, both of them often coexisting in ICU patients.
In our routine we use 14-gauge single lumen CVCs, inserted with Seldinger technique and ultrasound assisted procedure, effective in 95% of the effusions and less invasive than a pleurocath (that we use most of the times for pneumothorax) or a real chest tube, which I keep for blood or traumatic pneumothorax.
Greetings from Italy,
Marco
Glad to hear it Marco! I started with CVCs as well before we were able to find inexpensive pigtails – email me for info if you want I don’t want to “brand” these things! They are actually really good because I found CVCs would often occlude. Patient comfort with either is so much more than chest tubes.
Great point about the “michelin man” who is very “wet” but intravascularly dry, which we see commonly post acute phase of critical illness, especially when physicians are so keen to use crystalloids.
thanks for reading!
Philippe
Hi Philippe,
I am very happy to read your post tonight, bacause I am part of that 15% and luckily most of my colleagues are in the same group. I agree in particular when you say that pleural effusions are the last to resolve, being the most “distal” to the circulation. I often find patients, at a certain point during their ICU stay, be not only like a “michelin man” but also (and at the same time!) hypovolemic. I call this situation, when I try to explain it to residents, “empty in full” (maybe in english it doesn’t sound as good as in italian): we are trying with diuretics and some fluid restriction to manage those extravascular fluids that prevent weaning from mechanical ventilation, but often we get the only effect of causing renal failure rather than eliminating pleural effusions. In this case the only way is to drain.
Another important point is that bedside chest x-ray is absolutely useless when you have to discriminate between pleural effusion and parenchimal consolidation, both of them often coexisting in ICU patients.
In our routine we use 14-gauge single lumen CVCs, inserted with Seldinger technique and ultrasound assisted procedure, effective in 95% of the effusions and less invasive than a pleurocath (that we use most of the times for pneumothorax) or a real chest tube, which I keep for blood or traumatic pneumothorax.
Greetings from Italy,
Marco
Glad to hear it Marco! I started with CVCs as well before we were able to find inexpensive pigtails – email me for info if you want I don’t want to “brand” these things! They are actually really good because I found CVCs would often occlude. Patient comfort with either is so much more than chest tubes.
Great point about the “michelin man” who is very “wet” but intravascularly dry, which we see commonly post acute phase of critical illness, especially when physicians are so keen to use crystalloids.
thanks for reading!