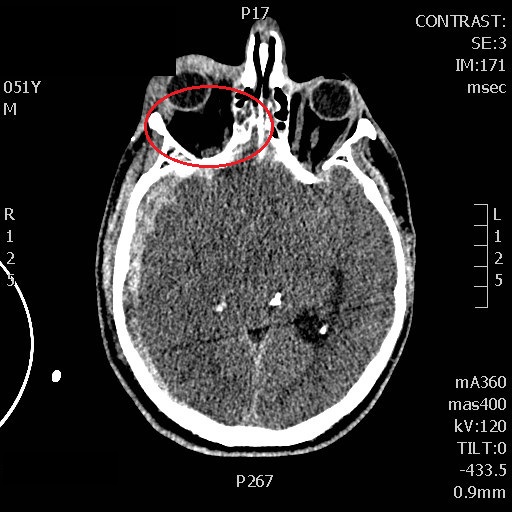
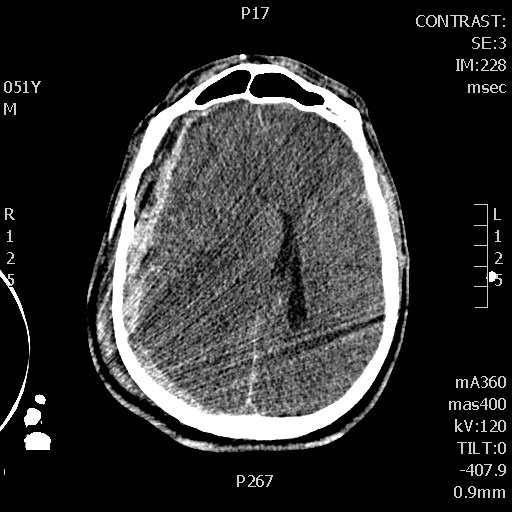
So a few years ago I had a patient in the ICU, post op for some abdominal surgery, and, using POCUS, I detected a hyper echoic area in the liver, in a wedge shape. I scanned the patient and, lo and behold, there was a matching area of air-filled hepatic venous sinuses on CT scan. Well, my surgical colleague and I were very concerned and proceeded to inform the patient he would be needing exploratory surgery for what was likely ischémie bowel. He essentially – though in more polite words – told us we were idiots and that his belly felt fine and he didn’t think surgery would be needed at all.
His belly did feel fine. So were his labs. So we worried, but, given this whole thing about free will and consent, etc, couldn’t very well force him into what we felt was necessary surgery.
The next day he was fine. On POCUS, the area of air had shrunk. The next day, it was gone altogether.
We thanked him for his keen clinical acumen and for teaching us a good lesson.
However, we were a bit perplexed, because traditional teaching equated portal venous air with a severe bowel disorder, usually ischemic or inflammatory, with exceedingly high mortality. At least that is what we had been fed. We are both grads of 1999. Hmmm…
So over the next few years we saw a few of these cases, sometimes bad, sometimes not, and a review of the literature (see below) showed an interesting evolution of the disease. Described in the 1950’s on plain films, hepatic air was a bad omen indeed, with mortality in the 75-90% range. In the CT era, the mortality started to “drop” to the 35-60% range. Now you can find quite a few reports of “surprisingly” good outcomes with conservative management. So this evolution doesn’t represent a change in severity so much as the technological capability to detect smaller and smaller amounts of air in the venous system – just increased sensitivity. And now, with POCUS – ultrasound is the most sensitive detector of air in a vascular tree – the associated mortality is likely to take another drop, not only because of our ability to detect very small amounts of air, but also because we are actually looking at the area, and also in a wider range of patient’ pathologies that those commonly associated with HPVG.
Clinical Case: HPVG and PE!
So a couple weeks ago I saw a patient in the ED who’d recently broken an ankle, had her foot put in a boot and managed conservatively and came back dyspneic and tachycardic. Here are a couple of clips:
As always, I start with the IVC:
Big & fixed.
Hepatic veins:
Biphasic flow.
Femoral veins:
So here the source of the problem is pretty clear, a large common femoral DVT.
She wasn’t very echogenic so I don’t have great clips of the heart but she had a dilated and hypocontractile RV with a McConnell’s sign (preserved apical contraction), small and hyper dynamic LV with septal flattening.
Now here is where it gets interesting, the portal vein:
You can clearly see bubbles traveling up the portal vein. Ominous, or not?
So clinically, her abdomen was normal, she had no abdominal symptomatology at all…
Pathophysiological musings:
So the severe RV obstruction resulted in significant venous congestion. Additionally, the decreased cardiac output – as manifested by a lactate of 4 and mild tachycardia/hypotension (110 HR, BP sys 90’s) was clear.
The etiology of HPVG in the literature isn’t clear – mucosal disruption, bacterial gas are all mentioned but as far as I could find, no definitive answer.
Is it possible that there is a “normal” inward leak of mucosal gas that is normally fully dissolved in the venous bloodstream, but that, in cases of low flow and/or venous congestion, the dissolution capacity (per unit time) decreases, and that gas comes out of solution? Alternately, those who have increased intraluminal pressure (gastric distension, etc), the increased transmembrane gas driving pressure may overload an adequate blood flow…
This would explain the benign course of many patients, particularily those with gastric dilation.
Clinical course:
Based on hemodynamics, tachypnea and, to some degree, venous congestion, I decided to thrombolyse her using 1/2 dose lytics. Within a couple of hours her HR decreased to the 90’s and BP rose to 110 systolic. Echographically, however, the IVC/RV findings remained similar, but the HPVG decreased. By the next day, HPVG was altogether gone, lactate had resolved and dyspnea was significantly better.
Take Home Message:
HPVG, although not quite as poor a prognostic sign as once thought, nonetheless warrants concern and investigation, even if the abdominal exam is entirely normal and without symptomatology, as correction of an underlying cause of “benign” HPVG (whether low-flow or bowel distension) would still need to be addressed.
In the meantime, I suspect that, reported or not, this has been noted by other POCUS enthusiasts, since we are now looking more frequently at this area, and are dealing with patients with low-flow states, congestion, bowel obstruction/ileus or more than one of these.
Hopefully some investigators will take a look at this phenomenon and delineate the pathophysiological mechanism!
Love to hear of your experience with this.
cheers!
Philippe
For those interested in POCUS, see here for a quick read primer on clinical applications of POCUS.
HPVG Review article 2009: