First of all, happy holidays to all and happy new year!
Following a few requests, I’m gonna put up a few words about the N=1 concept, as I think it comes up in every single therapeutic and diagnostic strategy.
We do not treat a thousand, a hundred or even ten patients at a time. As clinicians, we deal with a single patient, with a certain pathology, and his own, unique physiological pattern of response to that pathology.
In a medical utopia, we would be able to have a precise biophysiological profile of our patient – probably including parameters that either don’t yet exist, or are on the verge of being found or invented. We would know, for instance, the degree of glycocalyx damage, the nature of this damage, the degree of subsequent capillary leak, the specific inflammatory cytokine pattern, and thus be able to use a potential combination of agonists and antagonists to favor healing, and tailor fluid therapy to the “just right” amount, avoiding both under-resuscitation and tissue edema. This would be similar to antibiotic sensitivity testing. Who, in this century so far, would deliberately not order sensitivities, instead satisfying themselves with a positive result and happy with empiric therapy?
Just in terms of biological variability, it is impossible to believe that all patients would respond best to a single goal or therapy. How can an MAP of 65 be as good for a septic hypertensive patient as it is for a young septic woman who normally walks around with an SBP of 110? Not that I don’t use that number myself most of the time, but certainly food for thought, and something to keep in mind when treating either of those “types” of patients…
And the answer to the N=1 riddle isn’t just subgroup analysis. The questions have to be answered in prospective fashion, built into the study design. Not easy work, and especially since we don’t yet even know what the key variables/questions are… But personally, as mentioned in an earlier post, I do now suspect that the ubiquitous glycocalyx holds some of those answers.
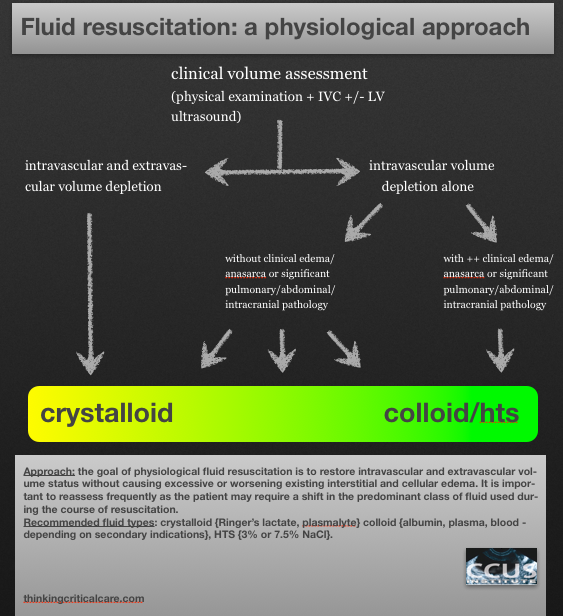
Let’s look at the whole fluid debate through the N=1 lens: it makes no sense whatsoever to debate crystalloids versus colloids. This negates thinking and only encourages near-religious fervour amidst both camps. Rather, look at your patient. Is he truly dehydrated/volume depleted or just volume responsive on the basis of vasodilation. If we want to restore the ICF and the interstitium, then crystalloids are probably better, but if we want to restore effective circulatory volume, then some measure of colloid may help avoid excessive edema, though even this can be debated. Even more important is the composition of the resuscitation fluid. Much as we adjust our TPN, we should probably design our resuscitation fluids, rather than only using Ringer’s Lactate (I say only just to drive the point that NS should not be used as a resuscitation fluid, unless repleting chloride is specifically necessary).
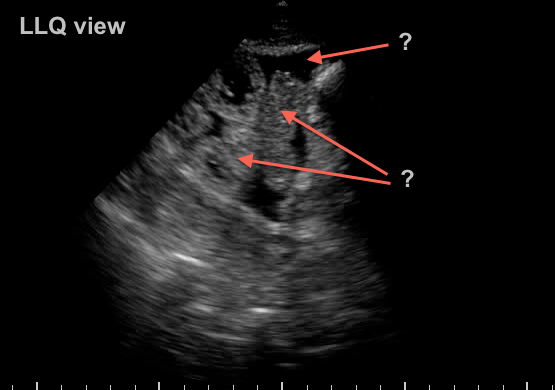
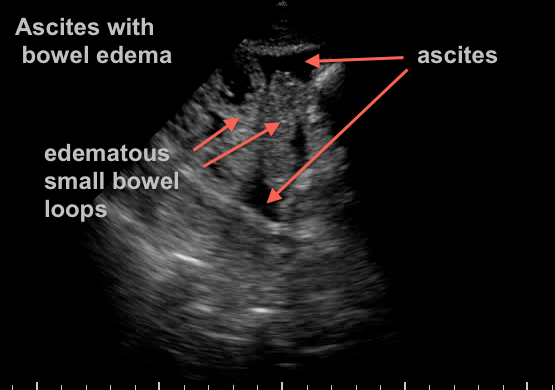
Now this may sound like a rant against large trials, but it isn’t. Absolutely invaluable information can be derived from these, it is just a matter of thinking how that information can benefit the one patient you have in front of you. And this isn’t easy. You have to put together your history, physical exam, bedside ultrasound exam and labwork. You can’t just say “sepsis? 2 litres,” or any other such recipe (aka protocols).
ok, enough for a january 1st!
Love to hear what anyone thinks!
Philippe