I was recently scanning the literature in preparation for our symposium, and came across what should have been a 2003 instead of a 2013 publication in the March issue of the CCM Journal, entitled “Point-of-Care Ultrasound to estimate Central Venous Pressure: A Comparison of Three Techniques.”
I have to admit this is a pet peeve of mine, from the standpoint of a clinical physiologist, which is, as far as I’m concerned, what any physician looking after critically ill patients should be, at least some of the time.
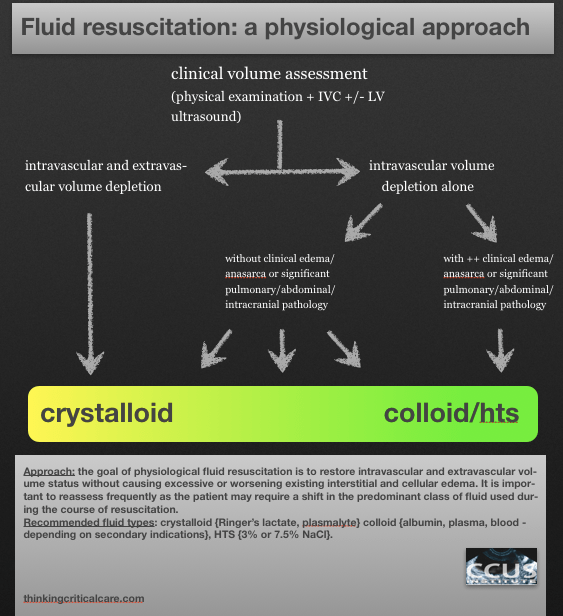
So our real question is: is my patient fluid-responsive? And perhaps a corollary question would be: is he fluid tolerant?
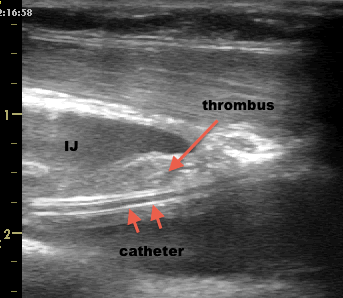
As a longtime bedside sonographer, physiology, experience and slowly growing evidence all support my using IVC sonography as a tool to assess volume responsiveness. It isn’t perfect, and personally, I find the common M-mode, two-point measurement to be inadequate compared to a global assessment of the IVC, but it certainly is far closer to “the truth” we seek than CVP.
This then begs the question: why on earth would we be seeking to correlate one type of data to another which is clearly more removed from “the truth” we seek?
The use of CVP is largely cultural and deeply ingrained. There are some limited ways and pathologies in which it can be useful, but not as a measure of preload. My friend Paul Marik published a piece that was both enlightening and entertaining in Chest a couple of years ago which I would have thought would have been the final nail in the coffin for the use of CVP as a preload tool, but it endures…even in the latest surviving sepsis guidelines…
A testament to religion over science.
Philippe Rola
http://www.ccusinstitute.org
note that this was first posted in my buddy Matt’s awesome website pulmccmcentral (http://pulmccm.org/2013/critical-care-review/why-do-we-bother-to-check-cvp/) please check it out!