So I get a call from a colleague in the ED at about 2am, telling me about a 39 yr old woman post-arrest. So I start putting on my boots and warming up the car (it’s January in Montreal folks). Apparently she had presented earlier in severe acidosis, the diagnosis is unclear, but she apparently got 2 units for an Hb of 49, then went into respiratory failure and got intubated. She arrested about 30 minutes later, cause unknown.
I tell the ICU to prepare a bed but I want to see her in the ED first. Twenty minutes later I put probe to patient and see a full IVC with spontaneous echo contrast. On that I tell the nurse to hold the fluids – there was a bag and tubing and a pump with 100ml/hr on it – and turn into a subxiphoid view to see a normal RV and a hypokinetic LV with some WMAs. She has marked consolidations in both posterior lung fields and B lines laterally, with small effusions and dynamic air bronchograms (indicating patent airways). At this point she has a HR of about 120, but there is neither perceptible BP (by NIBP) nor saturation. She’s on levophed at 20mcg. She’s about an hour post arrest which was witnessed and brief (<10min to ROSC).
The theories about the arrest are possible hyperkalemia: she was intubated with succinylcholine before the K of 6.1 was back from the lab, and her pre-intubation pH was 7.0, and post-intubation she was only ventilated at 400 x 18, possibly precipitating a drop in pH and a rise in K. Her EKG had some nonspecific signs at this point, but also a poor anterior R wave.
So we head to the ICU, as instrumentation was needed. Cerebral saturation (SctO2) is 42% and ETCO2 is 20mmhg, which reassures me that the BP is probably in the measurable range (normal SctO2 is >60% and varies, but 47% is certainly viable)… A jugular CVC with continuous ScVo2 and a femoral arterial line goes in:

So with a BP of 59/44 (ignore the 100/46, not sure whose arm that was on!) I start epinephrine, as the POCUS is similar, as I want some added beta-agonism. ScVO2 matches SctO2 in the 40’s. We get the BP up the the 90-1oo range, the ETCO2 goes to 30, the SctO2 and ScVo2 go up into the high 40’s, which is very reassuring, because with this I know that my epi drip is improving perfusion and NOT over-vasoconstricting. Without looking at a real-time tissue perfusion index of some sort or other, it is nearly impossible to know rapidly whether your therapy is helping or harming (will discuss tissue saturation & resuscitation monitoring in more detail in another post sometime soon).

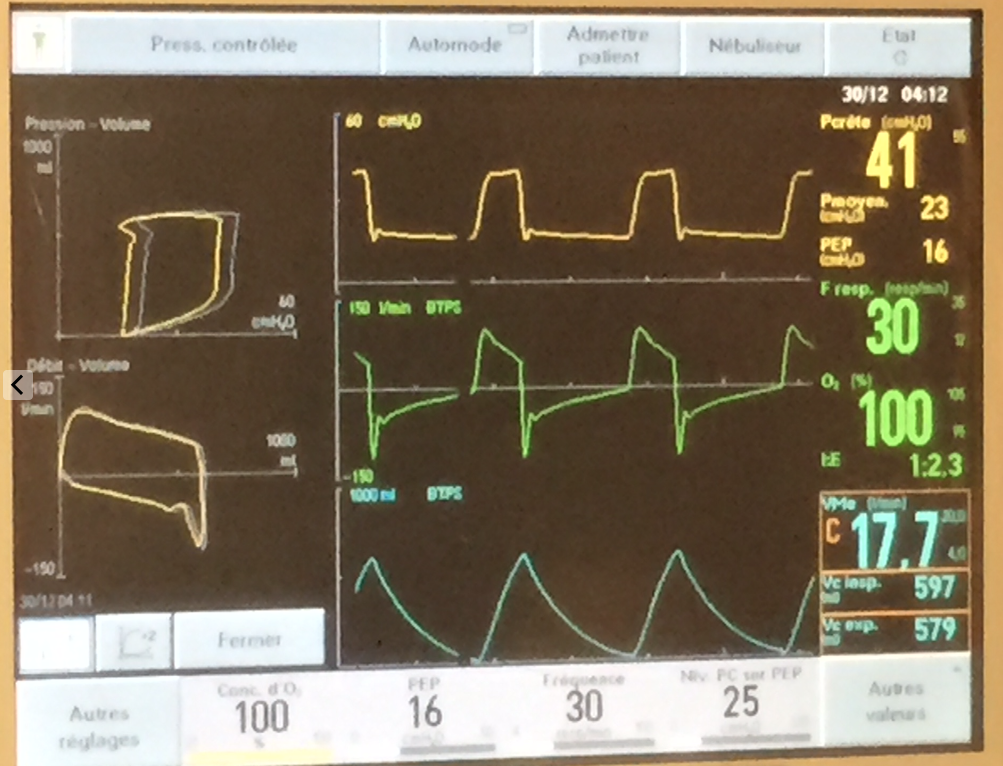
So now the sat finally starts to record in the low 60’s. We have a PEEP of 5, so start bringing it up. We hit 16 before the BP starts to drop, and that only gets us to the mid 70’s sat%. She actually squeezes my hand to command.
At this point I take a few seconds to recap in my mind. I’d spoken to the husband briefly and she had had recurrent episodes of feeling unwell with headache, nausea and diaphoresis, and that had been out for dinner earlier and she felt fine until later in the evening when this came on and eventually brought her to hospital. There was also a notion of hypertension at an ER visit a couple of weeks ago. Her history was otherwise not significant. Nonsmoker.
Pheo? Maybe, but shock? I repeat the EKG, and now, in I and AVL, there is perhaps a 1mm ST elevation. She’s 39 and essentially dying. Lactate comes back >15, pH 6.9. I give her a few more amps of NaHCO3. You can see the BP respond to each amp. I decide we need to go to the cath lab and get the cardiologist on call to get on the horn with the interventional team at a nearby hospital with a cath lab and ECMO, which is what I think she needs. Hb comes back at 116, making that initial 49 that prompted 2 PRBCs probably a technical or lab error…very unfortunate. There are no visible signs of significant bleeding.
But back to the patient, because this isn’t really a transferrable case.
Recap: a 39yr old woman in cardiogenic shock AND in severe congestive heart failure exacerbated by fluids and packed red cells, with a PO2 in the 40’s and sat in the 70’s.
So I decide to prone her.

Along with draining tamponades, this had to be one of the most rapid and rewarding maneuvers I’ve done. There was a scry drop of sat to the 40’s for a few seconds (may have been a technical thing), but then within a few minutes: BP to the 130’s, SctO2 to 59% and sat 100%!



We dropped the vasopressors, the FiO2, and all breathed a collective sigh of relief. Now for the novices out there, prone ventilation improves VQ mismatch by moving perfusion from diseased, posterior lung fields to now-dependant, relatively healthy, anterior lung fields.
So transfer at this point was in the works. I planned to leave her prone until the last minute. The miraculous effect started to slowly wane within about 30 minutes, with sat and BP creeping down. At the time of transfer, we were back up to 80% FiO2.
So why is this? Simple enough, this being simple pulmonary edema – rather than consolidated pneumonia – it migrated to dependent areas relatively quickly. This was confirmed by a quick POCUS check:

So in the still shots, you see a pristine “A” profile (normal, no edema) from the patient’s back, and a severe consolidation or “C” profile with ultrasound bronchograms in the antero-lateral (now dependant) chest. Impressive. (for those wanting some POCUS pearls see other posts and here). This is the reverse of her initial POCUS exam.
So we flipped her back and transported her – lights & sirens – the the cath lab, where they were waiting with ECMO cannulae. As an aside, it was quite refreshing to speak to the ICU fellow who spoke POCUS as well as french and english – it’s not usually the case, but I’m glad to see the change. I do believe it to be a direct effect of the influence of my friend and mentor, Dr. Andre Denault, one of the POCUS deities.
So she turned out to have a normal cath and a large adrenal mass. She did well on ECMO, being weaned off it today, and is now alpha-blocked and waiting for surgery, neurologically intact for all intents and purposes. A big thanks to the interventionists and the ICU team at the Montreal Heart Institute. Puts a smile on my face.
Take Home Points:
- don’t resuscitate without POCUS. I wouldn’t want anyone guessing with my life on the line, would you?
- keep pheo in mind as a cause of “acute MI” and shock
- if you’re not using some form of realtime monitor of perfusion (continuous CO, SctO2, ETCO2, ScvO2) then all you’ve got is looking at the skin and mentation, so you are essentially flying blind. Lactate and urine output are not realtime in real life.
- get ECMO in the house, it’ll come in handy. I’m working on it.
Love to hear some comments!
cheers
Philippe
ps I’ll try to add more ultrasound clips from this case in the next few days.