First of all, I would like to commend those involved in the Surviving Sepsis Campaign’s Guidelines. It is a tremendous endeavour that, without a doubt, has heightened awareness and their growing implementation has and will save many lives.
I would, however, also like to point out that guidelines are exactly what the term implies, and not necessarily a gold standard to aspire to and adhere to in religious fashion. The reason this is so is the inherent variability in human physiology and pathology. If, out of 100 patients a treatment would help 10 but harm 1, the numbers and studies would clearly support its broad use. We’d win more than we’d lose. However, as physicians, we treat the one patient in front of us, not the hundred, so I find it difficult to believe that such blind application of a recipe would be the most Hippocratic practice to apply.
We know that our patients are widely different, and around the corner is point of care immunology that will tell us, in all likelihood, that even patients we think are similar on the surface will have widely different immune profiles and will respond to treatment differently.
There are a few recommendations which, to me, make little physiological sense, particularly in certain circumstances:
I don’t think it necessary to belabour the point about CVP. As a static measure, CVP has clearly been disproven to have any relevance in predicting volume responsiveness. Its persistence is a testament to cultural faith rather than science.
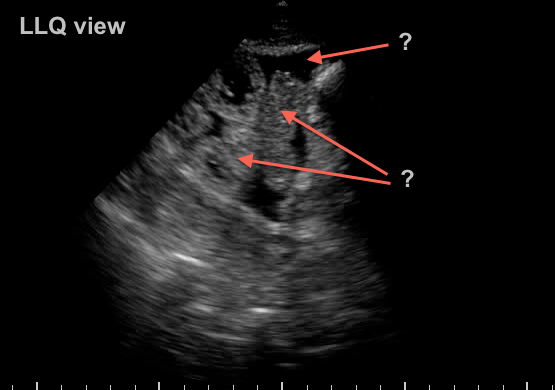
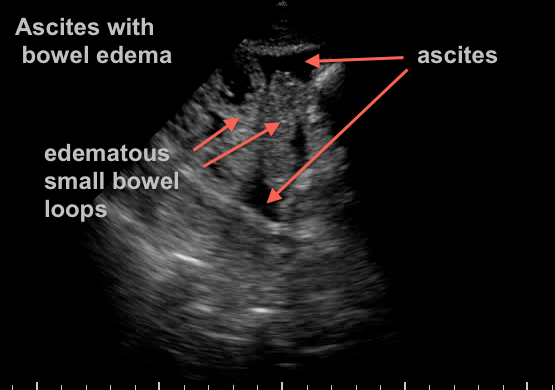
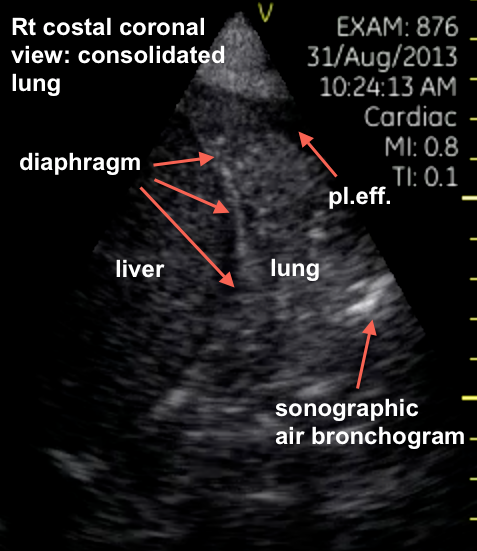
I would find it unethical to blindly bolus large amount of crystalloids (which we all know end up 70-80% extravascular) in a patient when it takes about 10 seconds to rule out a pre-existing, septic cardiomyopathy or a volume-intolerant state. Even more so when dealing with pathologies where third-spacing is a concern (pulmonary and intra-abdominal pathologies) since those leaky capillaries is where most of that fluid resuscitation will end up. Yes, I am implying that a worsening chest x-ray is not always and only due to worsening disease… Physiologically, perhaps non synthetic colloids or hypertonics may be a better option…
I would find it equally unethical to blindly put a patient on dobutamine who may have hyperdynamic ventricles and possibly still a volume-responsive state. Again, determining this takes seconds.
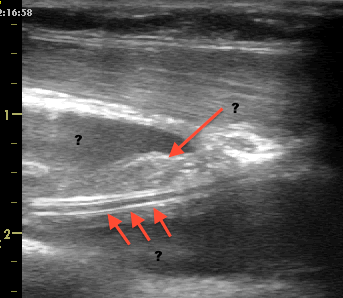
Yes, clearly I admit to a bedside ultrasound bias. It allows us to look inside our patients. Isn’t that what we’re always trying to do?
I can already hear voices and keyboards claiming the “lack of evidence,” and they would partly be right. That evidence is slowly but surely growing.
Unfortunately, point of care ultrasound has come of age in the era of evidence based medicine, and, as such, is required to “pass” that scrutiny whereas most of what is currently being done was “grandfathered in” and given a bye. I would be interested in seeing the compelling evidence for the use of a stethoscope.
The evolution of evidence based medicine is an interesting scientific, commercial and social development. From the positive study publishing bias to the general lack of epidemiological knowledge of our community, and without mentioning the darker side of research and publishing, it is unfortunate that almost every statement by a physician, to be taken seriously, must be backed by a hand raising a publication. And how many of those do we see torn down a month, a year or five later, thoroughly disproven? The pendulum of evidence-based medicine has perhaps swung too far…
Note that I’m not trying to discredit the countless number of truly well-designed and well-executed studies that contribute immensely to medicine – which would otherwise be reduced to little more than expert opinion – just that careful analysis of both the evidence and the case at hand is primordial.
I think that as physicians, it is our duty to look very closely at the individual patient, the care of whom we are privileged to have as a responsibility, and individualize our treatment plan to his specific problem given his specific physiology, and not blindly implement a recipe, even if it would happen to be the right one 9 out of 10 times.
Philippe Rola
http://www.ccusinstitute.org
please note that this was first posted on september 5th, 2013 on my buddy Matt’s website, pulmccm.org (http://pulmccm.org/2013/uncategorized/surviving-sepsis-guidelines-useful-patients-deserve-individualized-care/)
Go visit, its great, and you can see some fun follow up comments, too!
Glenn says:
it’s a sensitive decease in a sensitive time. Time is of the essence in treating septic shock and severe sepsis. If you wait for primary MD to individualized the care for these patients,it’s probably too late.EGDT save lives.
Thanks for commenting Glenn, and I can’t agree more. EGDT does save lives when compared to the usual care of 2001 (see my latest post on the ProCESS trial as that may no longer be the case in some institutions), but the mistake is strict adherence when you do have the capabilities to detect conditions where a protocol “violation” would be beneficial to the individual patient in front of you. Again, I’m not knocking EGDT, it was a great step, but in a set of stairs we have to keep climbing.
Philippe