
So I’ve been quite passionate about adding ECPR to our shop for quite a while now, but bureaucratic hospital processes, particularly in Quebec these days, has us bogged down and makes progress slow and painful, despite good intentions. So we need a boost, not only to be able to offer this technology to our patients, but more importantly, to show that it can be done in a community hospital, that all you need is the desire to give your cardiac arrest patients the best chance at neurologically intact survival they can get.
Here’s a little explanation, particularly for the non-medical readers:
That, and of course a pre-determined corridor to a tertiary care center with a cath lab and a compatible ECMO system to yours.
We have the good fortune to be a couple blocks from the Montreal Heart Institute who are interested in collaborating, and we have the desire, skill and motivation to pull this this off.
It’s important for both MDs and non-MDs to understand that this approach would possibly save 50% of the patients that we normally have no hope to save. At the point when we initiate ECMO, these patients have almost no chance with the current means. That is an incredible impact.
But we do need your help. The government isn’t moving fast, and won’t until this is established practice (well Dr. Rola, where else is this being done locally? – same question/answer as when I asked for a 100,000$ ultrasound system for our ICU in 2004: nowhere around here!).
So I figured that if we can raise enough money, and with the help of our awesome Foundation – under the presidency of Mr. Arcobelli, no effort has been spared to raise funds and the quality of care that we offer at Santa Cabrini! So to help them out and to get the ball rolling, we’re setting up our project on chuffed.org, a crowdfunding site which is tied to the Santa Cabrini Hospital Foundation, and every dollar will be specifically earmarked for this and not used for anything else.
My hope is that by the end of 2019, we have an active ECMO unit able to be deployed for cardiac arrest cases in the east end of Montreal, and that in the years following, other community hospitals follow suit. We are a small community hospital, but with a big heart!
We need 250,000$. The device costs about 150,000$, each circuit about 7,000$ and we need to set up some training for the team. That should get us jumpstarted and cover the first 10 patients.
We’re more than happy to field any questions. As a start, the Critical Care & Ultrasound Institute be donating a minimum of 2,000$ (it’s a bit early to be able to commit to more, as we do have to feed the participants and bring the faculty…) from the H&R2019 conference, , which takes place at Santa Cabrini Hospital from May 21-24, 2019.
I’d like to thank Joe Bellezzo, Zack Shinar and Scott Weingart from the @edecmo project who planted the seed and showed all of us that this could be done.
for those who want to know more:
I would also like to thank Santa Cabrini’s Team 6444 of operators, who are a major driving force behind this effort: Sandy Mormina, Rita Pisanelli and more!
PLEASE HELP AND DONATE AT: http://www.chuffed.org (not active yet, will be linked soon) and please forward this to friends and colleagues. You can also send a cheque labelled “ROLA ECMO Project” in the note part of the cheque (this will ensure that the money cannot be used for anything else) to the following address:
Santa Cabrini Hospital Foundation, 5655 Rue St-Zotique, Montreal, H1T1P7, QC, Canada.
Every dollar gets us a little bit closer!
cheers and thank you!
Dr. Philippe Rola
Chief of Service, Intensive Care Unit, Santa Cabrini Hospital


















So, fresh from reading Jon’s post, I felt I had to add a bit of nuance in my previous post to what I feared some might extract as a take-home message, even if in fact, we are not that differing in opinion at all – which Jon expressed here:
i agree with ultrasound for finding the uncommon causes of shock. these examples seems to permeate twitter and make ultrasound very appealing. because ultrasound is non-invasive, it makes the risk-to-benefit ratio very low for these uncommon but highly-lethal and treatable causes.
but that needs to be compared to the risk-to-benefit ratio of ultrasound for the more common causes of shock – like ‘non-cardiogenic, septic’ etiologies as seen in SHOC-ED. here, “static’ ultrasound [as per the RUSH and ACES protocols] – per SHOC-ED – appears to be neither helpful nor harmful. your read of the discussion is perfect, but i was depressed because it read as if the authors only realized this ex post facto – study of previous monitoring utensils [e.g. PAC] should have pre-warned the authors …
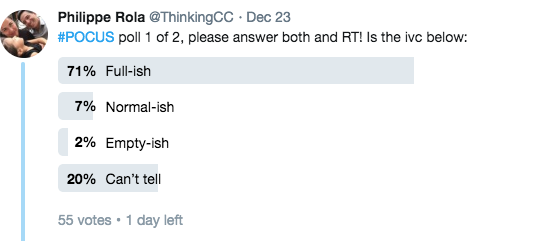
i will take some mild issue with markers of volume responsiveness and tolerance. you are correct on both fronts – but what the data for the IVC reveals – perhaps paradoxically – is that true fluid responders can have a very wide-range of IVC sizes from small to large and unvarying … this was born out in most of the spontaneously breathing IVC papers [airpetian and more recent corl paper] the sensitivity was rather poor.
the same *could* be true for the opposite side of the coin. a large great vein may not mean a volume intolerant patient. i tried to exemplify how that could be so in the illustrative case in my post. an elderly man, with probable pulmonary hypertension and chronic TR who probably “lives” at high right-sided pressures. nevertheless, he likely has recurrent C. diff and is presenting 1. hypovolemic and 2. fluid responsive despite his high right-sided pressures. portal vein pulsatility *could* be quite high in this patient – but he still needed some volume.
the obvious underlying issue here – which I know you are well attuned to – is that a Bayesian approach is imperative. when you PoCUS your patients, you are inherently taking this into consideration – i know that you are a sophisticated sonographer. my hidden thesis of the post is that if ultrasound findings are followed in a clinical vacuum and followed without really understanding the physiology [which can explain clinico-sonographic dissociation – like the patient in my fictitious case]… disappointment awaits.