
Just a clip.
What’s the dx?
scroll below!
sinus tachycardia with 3rd degree HB – taken on a call on the ward before the tech brought the EKG machine.
thought it was neat.
Philippe
Just a clip.
What’s the dx?
scroll below!
sinus tachycardia with 3rd degree HB – taken on a call on the ward before the tech brought the EKG machine.
thought it was neat.
Philippe
Ok, so it was pretty cool to see an NEJM issue basically dedicated to septic shock management, I must admit. But let’s dig a little deeper, shall we?
So here is where they are: http://www.nejm.org, and fully available for now.
I won’t go through all the details and numbers, after all they are in the papers, so let’s just analyze them from two principles:
a. the N=1 principle – how was therapy individualized?
and
b. was there any integrated monitoring of the therapeutic goals?
…and we’ll conclude by looking at the potential practice-changing potential of each of these studies.
So first of all,
High vs Low BP Target in Septic Shock, by Asfar et al.
So basically a negative study except for two findings, the increased incidence of afib in the high target group and the decreased need for renal replacement therapy among chronic hypertensives in the high target group.
so N=1 is not really revealed:
“Refractoriness to fluid resuscitation was defined as a lack of response to the administration of 30 ml of normal saline per kilogram of body weight or of colloids or was determined according to a clinician’s assessment of inadequate hemodynamic results on the basis of values obtained during right-heart catheterization, pulse-pressure measurement, stroke-volume measurement, or echocardiography (although study investigators did not record the values for these variables).”
So lets just hope that the variability evens itself out between the groups, since we don’t really know. The numbers don’t really tell the tale, because the average fluids received (10 liters over 5 days) could mean one patient got 15 and one got 5 – although let’s trust they followed the French Fluid Resus protocol…
So the atrial fibrillation makes total sense – more B agonism should result in that, and the decreased renal failure also does.
As the authors note, the actual BP averages were higher than planned. For those of us practicing critical care, we know most nurses titrating prefer having a little bit of extra BP – even when I prescribe MAP 65, I usually see the 70 or so unless I make a point to tell them. Understandable. They also note the underpowered-ness of their own study, but I think it is still worth looking at their results.
So…bottom line? I think it’s a great study for a couple of reasons.
The first is to remind us to pay a little more N=1 attention to the chronic hypertensives, and that it is probably worth aiming for slightly higher MAPs.
The second, debunking the myth of “levophed, leave’em dead” (which I heard throughout residency at McGill), and the concept of doing everything (ie juicing patient into a michelin man) in order to avoid the “dreaded and dangerous” vasopressors. So really I think an alternative way to conclude this study is that it isn’t harmful to have higher doses of vasopressors. I think this is actually a really good study on which to base assessment of more aggressive vasopressor support vs fluid resuscitation, in the right patients.
It would have been interesting to have echo data on those who developed a fib – were they patients who had normal to hyperdynamic LVs who in truth did not need B agonism at all and would have been fine with phenylephrine? Perhaps…
Cool. I like it.
Next:
Albumin Replacement in Patients with Severe Sepsis or Septic Shock, by Caironi et al. The ALBIOS study (a Gattinoni crew)
So basically showed no difference, so pretty much a solid italian remake of the SAFE study in a sense, confirming that albumin is indeed safe overall, and may be better in those with shock. As the authors note, mortality was low, organ failure was low, so study power a little low as well. Note the mean lactates in the 2’s at baseline. The albumin levels of the crytalloid only gorup were also not that low, low to mid 20’s, whereas I often see 15-20 range in my patients, especially if I inherit them after a few days, as I do use albumin myself a fair bit. They also used a target albumin level, not albumin as a resuscitation fluid purely.
In my mind the benefit of albumin would be greatest in those with significant capillary leak, particularly those with intra-abdominal and pulmonary pathology. It would have been nice to see a subgroup analysis where extravascular lung water was looked at (especially coming from a Gattinoni crew!).
Another interesting thing would have been to know the infusion time of the albumin, since animal data tells us that a 3hr infusion decreases extravasation and improves vascular filling vs shorter infusion times. I routinely insist on 3hr infusion per unit, which sometimes results in 9-12hr infusions, almost albumin drips!
Bottom line?
I like it. Reinforces that albumin is safe, so makes me even more comfortable in using it in the patients where my N=1 analysis tells me to be wary of third-spacing. Also the fact that they used 20% – in Canada we have 100cc bottles of 25% for the most part – is nice, since the SAFE data used 4%.
Next!
A Randomized Trial of Protocol-Based Care for Early Septic Shock – The ProCESS Trial.
So right off that bat my allergy to protocols flares up, so I’ll try to remain impartial. It just goes against the N=1 principle. The absolutely awesome thing about protocols is that it primes the team/system to react – so clearly protocols are better than no-protocol-at-all, but strict adherence would clearly not fit everyone, so that some built-in flexibility should be present.
This being said, the ProCESS study is really interesting, for a number of reasons. They have three groups, and compare basically (1) Rivers’ EGDT to (2) their own protocol (see the S2 appendix online) which gives a little more flexibility and (3) “usual care”. Net result is that all are pretty equal, no change in mortality. As the authors note, their mortality was low, so again may not have been able to detect a difference.
So, what does this mean. To me it’s a little worrisome because I doubt that the “usual care” represents the true usual care found in EDs/ICUs all over the world, so I am concerned that many docs will use this as a reason to justify not changing their practice, similarly to many I’ve heard say they don’t need to cool anymore after the TTM trial. Human nature for some I guess.
Bottom line? You don’t have to follow EGDT if you’re conscientious and reassessing your patient frequently and have done all the other good things (abx, source control, etc). I think that’s really important because giving blood (see my post about S1P) to those with hb > 70 and giving dobutamine to patients with potentially normal or hyper dynamic LVs never made physiological sense to me, and the problem with a multi intervention study such as EGDT is that you can’t tease out the good from the bad or the neutral. Again, studies such as EGDT are pivotal in changing practice and raising awareness, so this is not a knock against a necessary study, just to highlight the point that each study is a step along the way of refining our resuscitation, and the important thing is to move on. In fact, the reason that this is a negative study is probably due to the improvement in “usual care” that EGDT brought along.
Conclusion: No new ground broken, but these studies do make me feel more confident and validated in continuing to not do certain things (strict EGDT) and doing others (albumin and earlier use of vasopressors).
Kudos to all investigators.
let me know what you think!
P
The usefulness of bedside ultrasound in cardiac arrest is clear, giving the clinician instant information on the hemodynamic process resulting in arrest. My arrest sequence is generally done as follows:
Step 1: IVC assessment
Step 2: Subxiphoid cardiac views
Step 3: Lung views if pneumothorax suspected.
Step 4: remaining views if possible (eg abdominal views to find source of bleeding, etc…)
The important part (as per current recommendations) is to have minimal interference on chest compressions. The IVC view, albeit jumpy, can generally be obtained during CPR. The subxiphoid view should be “prepared” during CPR, meaning that the sonographer warns the team member doing CPR not to stop compressions until he is told to do so (unless the team are already used to ultrasound in cardiac arrest), the probe positioned optimally, then instruction given to stop for five seconds while a look +/- loop is acquired. This should be enough to look for pericardial effusion, RV/LV ratio and LV contractility. In fact, experienced sonographers can usually get this while CPR is going on in many cases. Then CPR should be restarted. Hence for now, minimal interruptions in CPR (until the concept of “stutter CPR” really emerges!!!).
Here are a couple of views with active CPR:
In this case there is a clear RV overload with a dynamic but underfilled LV.
From the information obtained in those 5 seconds, one should be able to consider the need for volume (hypovolemia), thrombolytics (pulmonary embolism suspected) or drainage of fluid (tamponade) or air (pneumothorax). The possibility of an acute myocardial infarction must be considered as it is one of the most common causes but is difficult to confirm by ultrasound.
Pulseless Electrical Activity
This may be the most exciting area in which ultrasound will change management. In the absence of ultrasound, all PEA is more or less alike: there is organized electrical activity, but no pulse. Physiologically however, the range of diagnoses is very wide, with on one end, a perfectly good heart that is empty (hypovolemic shock in extremis), and on the other, cardiac standstill despite electrical activity. An astute physician does not need a randomized clinical trial to know that the management and prognoses of those two extremes are very different. Without bedside ultrasound, however, these would appear identical: “PEA.”
The heart rate cannot be relied on since it will largely depend on the phase (both would begin as tachycardic, then eventually bradycardic until asystole occurs).
Notwithstanding guidelines, the information obtained should be considered strongly. If we start by looking at the first end of the spectrum, there would be no physiological rationale for performing chest compressions or an empty and hyperdynamic ventricle: rapid infusers and vasopressors (to recruit venous unstressed volume) should be used instead. At the other end, the heart in standstill definitely needs compressions. Of course, there is then the whole range of varying RV and LV pathologies, tamponade, etc, all of which need to be dealt with individually. It is really a huge grey zone…
CPR or no CPR?
A very important question is whether CPR should or should not be performed in certain cases of PEA. Certainly ACLS protocol dictates so. However, ACLS has not yet truly integrated bedside ultrasound into management, only suggests in a very loose way – understandably since the protocols must be applied by all, and still only few use it regularly.
I have to credit Dr. Sue, an ER doc from Atlanta, who asked me the question about CPR in extreme hypotension, and I had to rewind in my mind the cases in which I had used physiological information to overrule the ACLS protocol in one direction or another and try to formulate an answer.
It is an excellent question and made me realize that there is no clear answer for two reasons:
One: PEA is not a diagnosis but a clinical syndrome. It relies on manual pulse check (unless the arrest occurs in a patient with an arterial line), hence the line between severe hypotension and true PEA is difficult to determine. Technically and physiologically speaking, if the LV contraction is sufficient to open the aortic valve, there is a “pulse.” Now how far along the arterial circuit this pulse travels is not known…unless it is monitored.
Two: The key question then becomes the following: at what level of endogenous blood pressure is the perfusion better than with “good” CPR? We do not yet have that answer. The coronary perfusion pressure (diastolic pressure – wedge pressure) data often quotes a minimal range of 15-25 mmhg, which – if we arbitrarily choose a high-ish wedge – would suggest we need a diastolic pressure in the 40’s (also note that that data is imperfect). Hence the arterial line. Perhaps there could be a role for tissue saturation/near-infrared spectroscopy or other microvascular flow indices in the future…
Now what about the huge spectrum of cases in between? Let us exclude the cases with immediately reversible causes such as tamponade and pneumothorax, where the initial management is clear, and instead focus on differing levels of RV and LV dysfunction resulting in the absence of a palpable pulse.
Predominant RV failure – although PE should be strongly suspected and thrombolysis considered, the question remains about management if you see a hyperdynamic but underfilled LV. CPR would appear reasonable in an effort to try to get some RV to LA flow. Endotracheal milrinone, sometimes used in cardiac anasthesia, can be an option as it provides inotropy and pulmonary vasodilation.
Predominant LV or biventricular failure – if cardiac activity is present, it seems imperative to start an infusion of vasopressors, and traditionally, do CPR until there is a measurable blood pressure. I have used CPR with progressing bradycardic rhythms for a few seconds to circulate the epinephrine, with at least short-term success.
Here is a typical LV “PEA” from the subxiphoid view:
Ideally, an arterial line would be very useful in these patients, and may help to decide on an individual basis when CPR should be used. Remember that CPR on a beating heart will likely worsen cardiac output as asynchronicity and increased mean intrathoracic pressure will impair filling.
Additionally, the arterial line also allows us to notice small trends during resuscitation, such as seeing that a few seconds of CPR may help circulate a bolus of vasopressor and enable it to take effect – progressive BP increase, or that the BP may be trending downwards despite vasopressor infusion – CPR may be useful until enough vasopressor/inotropes have infused.
Bottom Line:
1. if possible, put in an arterial line
2. bedside ultrasound is mandatory if you don’t want to miss anything reversible
3. if you don’t have a palpable pulse and your diastolic pressure (arterial line) is less than 40, consider some CPR until vasopressors/inotropes have had effect.
4. if you are lucky enough to have ECMO (shout out to Joe and Zack at http://www.edecmo.org) or other mechanical support, it would be the time to consider!
I think this is actually a really interesting area to develop, and I’d really, really like to hear what other sonographer-resuscitationists are doing, or what anyone else might think!
Philippe
Joe Bellezzo – yes, THE Joe, says:
Phil, I agree with all your points here. Great post! As you know, Shinar, Weingart and I recently published a rant on PEA (over at http://www.edecmo.org/13) and Weingart threw out two possible new monikers: PRE-M (Pulseless Rythm with Echocardiographic – Motion) and PRE-S (Pulseless Rythm with Echocardiographic – Standstill). I don’t disagree with any of those concepts but I think its simpler than that.
PRE-S (standstill) = asystole and you start compressions.
PRE-M (organized cardiac activity) = profound shock. In this setting I like the recent Littmann paper that gives a simplified approach (http://edecmo.org/wp-content/uploads/2014/08/A-Simplified-and-Structured-Teaching-Tool-for-the-Evaluation-and-Management-of-Pulseless-Electrical-Activity.pdf).
As you pointed out above, the real big question is at what point do you start compressions when you have cardiac motion? Your points above are spot on. The problem with compressions on a beating heart is that you don’t know what your end-point is. You lose the ability to do minute-minute diagnostics and doing any procedures with ongoing compressions is tough. And it seems to be a knee-jerk reaction for the RN or pharmacist to have an amp of epi ready to blast away at this point. NO!
I wait. I do stuff first. Step 1 is ECHO. If PRE-M (aka profound shock): EKG and arterial line NOW. Step 2: Stop, think and decide what you think is your top probable etiology of this profound shock and fix that. Step 3: reassess = repeat echo, EKG, and see what your art line pressures are doing. I try to do all that before I start compressions.
Example: “PEA” hits your door. Echo shows a wall motion abnormality and hypokinesis. EKG suggests ischemia but is not obvious STEMI. art line goes in simultaneously. I think this is MI. This heart does NOT NEED epi 1 mg! This is cardiogenic shock and I need to fix some stuff before I start pushing on the chest and blasting superhuman doses of epi! I usually start with a push dose epi (10-20 mics or so) while a pressor drip is prepped. Calcium bolus is given. I likely start dobutamine here (or milrenone if beta blocked). If that fixes your problem, then the pt goes to the cath lab. If it doesn’t, I cannulate and put the pt on VA-ECMO.
And what if I were wrong? what if this were a big PE? massive beta blocker OD? the protocol above is works in those cases too.
An aside, since you already placed a femoral venous line….and you popped in the Art line immediately, you have nice conduits to upsize to ECMO cannulas.
Great post Phil!
Thanks for sharing your approach! As you know and clearly show, a sensical physiological approach is absolutely needed in a day and age when we can (bedside ultrasound) see what’s really going on, and we can (ECMO) give these patients a fighting chance! See you at BMBTL in a couple of weeks!
Philippe
PS Joe (and Zack and Scott) will be talking about all this and more at CCUS 2015! http://www.ccusinstitute.org to register soon!
If you’re thinking of coming to Montreal to beef up your clinical skills and decision making, hurry up and register, we have to cap the participants to 100 (physical restrictions of the venue) and there aren’t too many spots left!
Myself, am looking forward to learning a bunch of things: how to diagnose bowel obstruction (Vicki Noble), how Andre Denault likes to integrate hemodynamic modalities in shock, how Mike (Stone) uses ultrasound to manage CHF patients, how Haney (Mallemat) uses it to manage abdominal pain, and many more…
Montreal, May 9-11, 2014, Santa Cabrini Hospital.
More info and registration at: http://ccusinstitute.org/Symposium6.html
See you there!
Philippe
Registration is open!
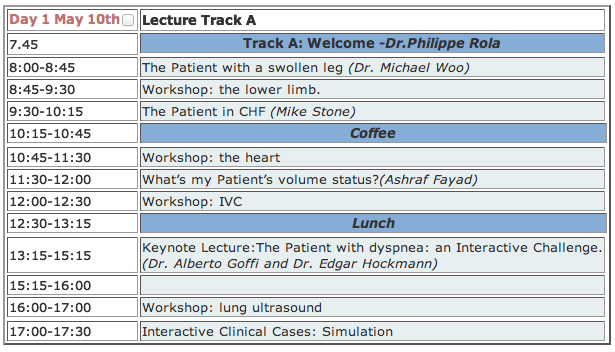
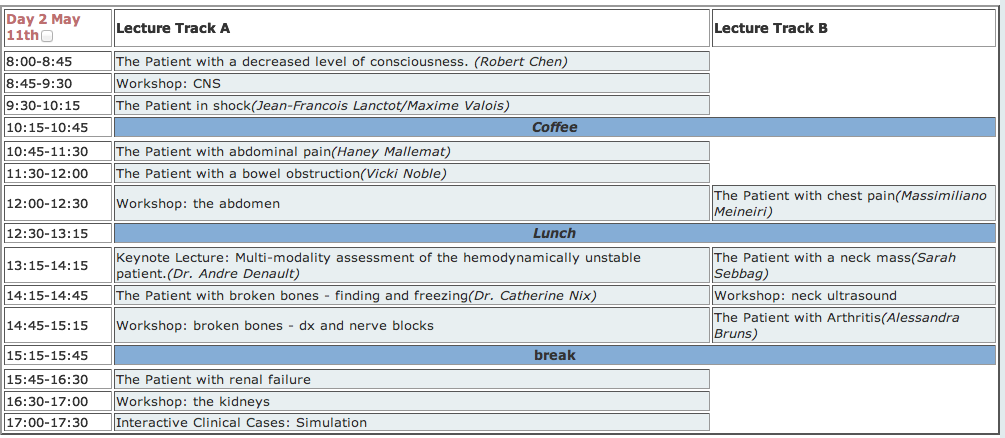
For the 7th edition of our Annual Symposium, we’ve assembled a great cast of characters to bring your bedside ultrasound game to a whole new level! Whether you’re a novice or have some experience in bedside ultrasound, we’re sure you’ll find our program very interesting, as the perspective we have chosen to take is patient-based, with each lecture explaining how ultrasound findings are integrated into clinical decision-making.
First of all, it’s in Montreal, May 10th and 11th, 2014. If you’re from out of town, its an awesome city to visit, and if you’re a Montrealer, well, it’s an awesome conference at home!
Indeed, this isn’t “just” a “how-to” course – although that is what we’ll be covering in the workshops which will follow each lecture – but a “how to integrate ultrasound into your daily practice” course, so no matter what your level is, you’ll find something suited for you. The workshops will be divided into novice and experienced and with a low participant to faculty ratio, will ensure a great experience.
So what are we going to be talking about?
In the CC/ED/hospital scene:
– the patient with chest pain, by Max Meineiri
– the patient with CHF, by Mike Stone
– the patient with renal failure, by Sara Sebbag
– the patient with a swollenleg, by Michael Woo
– what’s my patient’s volume status? By Ashraf Fayad
– the patient with a decreased level of consciousness, by Robert Chen
– the patient in shock, by JF Lanctot and Max Valois
– the patient with abdominal pain, by Haney Mallemat
– the patient with a bowel obstruction
– the patient with broken bones: finding and freezing, by Catherine Nix
– the patient with dyspnea, by Alberto Goffi and Edgar Hockmann (KEYNOTE)
– the hemodynamically unstable patient: multi-modality assessment, by Andre Denault (KEYNOTE)
In the office scene:
– the patient with a neck mass, by Sarah Sebbag
– the patient with arthritis, by Alessandra Bruns
Here is the program:
Who made this up? Our scientific committee is made up of Michael Woo, Catherine Nix, Edgar Hockmann, Alberto Goffi and Andre Denault, who is also the co-chair – with myself – of this year’s symposium.
For those of you part of the twitterverse and #FOAMed movement, you’ll get a chance to meet @criticalcarenow (Haney), @bedsidesono (Mike), @nobleultrasound (Vicki), @EGLS_JFandMax (JF and Max) and @ThinkingCC (yours truly)…and Matt (pulmccm.org) will be there to chronicle the event and bring the highlights to the #FOAMed world.
So who should come? Anyone taking care of sick patients. If you’re an ED doc, ICU doc, hospitalist, anaesthetist, surgeon, student or resident, this stuff is gold. Even if most of your practice is office-based, precise assessment of dyspnea, volume status and cardiac function is highly practical.
Additionally, there are several very interesting pre-congress courses taking place on May 9th, particularly the Echo-Guided Life Support course (JF Lanctot and Max Valois), a Bedside Ultrasound Course for Nurses, an Acute Care Procedures Course and a Symposium for Ultrasound Educators on how to set up training programs. All in all, a lot of great stuff.
For more details and registration, please go to www.ccusinstitute.org. And yes, of course there are CME credits by the University of Montreal.
As I said a few months ago – well, tweeted, to be exact – if you’re an acute care MD and NOT using bedside point-of-care ultrasound, you’re stuck in the 20th century… rude, but true.
Hope to see you there!
Philippe Rola
President, CCUS Institute
This, in my opinion, is an under-recognized problem when bedside ultrasound is NOT a routine part of examination of critically ill patients. I’m happy to say that as many of my colleagues have been picking up probes, it is somewhat less of an issue now, whereas a couple of years ago I’d often put in 4 or 5 pigtail catheters on day 1 of taking over the ICU.
The first and foremost reason for this is that the portable supine ICU CXR sucks at picking up the small to moderate to, yes, even the large pleural effusion. Largely owing to the fact that many of our patients have some lung parenchymal abnormalities and to the recumbent position that causes a layering of the effusion, it is often difficult to properly assess the size of a pleural effusion. Radiologists will usually report the presence of a probable effusion, but quantification is difficult, and physicians not performing routing bedside sonography will often realize the presence of a submassive effusion only on CT scan – after all it isn’t like you can turn and rotate your patient to percuss the shifting dullness, can you? Not very practical.
So the following can often be seen:

this is fairly large, or you might see:

So the obvious and critical question is: when is it necessary to drain?
There are two elements to this question:
a) for diagnostic purposes: unless the diagnosis is clear (eg CHF, post-resuscitation “michelin man” patient, etc) a new effusion should be tapped. Panapneumonic effusions, in particular, warrant ruling out empyema unless there is a compelling reason not to. For diagnostic purposes a 22g needle usually does the trick unless you have frank pus – which generally shows up differently on ultrasound.
b) for therapeutic purposes: effusions are space occupying lesions which compress the lung and result in a variable degree of respiratory compromise, depending on chest wall and diaphragmatic compliance, as well as effusion volume. The clinical effect is highly variable due to the above as well as the degree of parenchymal lung disease and the degree of PEEP. In the ICU or ED, a simple way to think about it is that if your patient is in respiratory failure and has a large effusion, chances are that draining it will improve things. It gets a little more controversial and complicated if you have a patient who is mildly dyspneic with a moderate sized effusion.
Here are a few clinical scenarios I like:
Mr. A is a 65 year old man with CHF, intubated, with large bilateral effusions. He has been aggressively diuresed to the point of his IVC being less than 5mm in diameter. He has not been able to wean in the last 48 h.
Yes, I definitely drain this fellow. Been there and done that time and time again. The pleural effusions are essentially the last to resolve (being the most “distal” to the circulation – vs the alveolar tissue itself) and hence can lag and cost a few more days or more of ventilation).
Mr. B is a 47 year old man with pneumonia, breathing spontaneously with a moderate (maybe 500ml) effusion. It appears free flowing and clear, he is afebrile with an improving white count, and mildly dyspneic.
Nah, I skip on this one. If fever and WBC recur, I do a diagnostic tap to r/o empyema.
Mrs. C is intubated on PEEP 18 FiO2 85% for ARDS due to pancreatitis. She has some degree of intraabdominal hypertension (IAP 18) and has bilateral moderate pleural effusions, maybe 400-500ml.
Yup. She can physiologically benefit from decreased intra-thoracic pressure, both from the ventilatory and the intra-abdominal pressure standpoint (Remember the diaphragm is not a rigid structure so that IAP and ITP are very similar in most cases).
So is there any evidence for this? Some. And that’s for part 2, coming within the next days. Part three will explain and show my procedure of choice for drainage.
Thanks!
love to hear what other guys’ practices are! Apparently only about 15% of ICU guys “routinely” drain effusions.
Philippe
COMMENTS
Hi Philippe,
I am very happy to read your post tonight, bacause I am part of that 15% and luckily most of my colleagues are in the same group. I agree in particular when you say that pleural effusions are the last to resolve, being the most “distal” to the circulation. I often find patients, at a certain point during their ICU stay, be not only like a “michelin man” but also (and at the same time!) hypovolemic. I call this situation, when I try to explain it to residents, “empty in full” (maybe in english it doesn’t sound as good as in italian): we are trying with diuretics and some fluid restriction to manage those extravascular fluids that prevent weaning from mechanical ventilation, but often we get the only effect of causing renal failure rather than eliminating pleural effusions. In this case the only way is to drain.
Another important point is that bedside chest x-ray is absolutely useless when you have to discriminate between pleural effusion and parenchimal consolidation, both of them often coexisting in ICU patients.
In our routine we use 14-gauge single lumen CVCs, inserted with Seldinger technique and ultrasound assisted procedure, effective in 95% of the effusions and less invasive than a pleurocath (that we use most of the times for pneumothorax) or a real chest tube, which I keep for blood or traumatic pneumothorax.
Greetings from Italy,
Marco
Glad to hear it Marco! I started with CVCs as well before we were able to find inexpensive pigtails – email me for info if you want I don’t want to “brand” these things! They are actually really good because I found CVCs would often occlude. Patient comfort with either is so much more than chest tubes.
Great point about the “michelin man” who is very “wet” but intravascularly dry, which we see commonly post acute phase of critical illness, especially when physicians are so keen to use crystalloids.
thanks for reading!
Philippe
So I just finished listening to the second podcast of The Resuscitationists’ Awesome Guide to Everything (www.ragepodcast.com), and as advertised, it is totally awesome. It’s really cool to have the point of view of several bright acute care clinicians whose field of expertise obviously overlaps but have different perspective in terms of experience and setting.
In episode 2, they do a great review of the MOPETT trial and thrombolysis in PE in general, and really work at distilling clinical information from academic literature, which is ultimately what has to be done. The hashing out of the finer points by using specific clinical scenarios is really, really good.
I have personally applied the MOPETT half dose TPA twice with good success, both in young patients and after explaining the risks and benefits. As in full dose thrombolysis, the clinical improvements in minutes to hours of massive/submassive PEs are quite remarkable.
So much kudos and everyone interested enough to read this should most definitely be checking them out, I know I’ll be!
thanks!
Philippe
So in my ongoing quest to reframe my resuscitation step-by-step, I’ve been following up on a number of leads regarding the glycocalyx, as previously stated, and John’s reference to this article in a previous comment I feel is highly relevant. So this is it:
Synergistic Effect of Anemia and Red Blood Cells Transfusion on Inflammation and Lung Injury, Anping Dong, Manjula Sunkara, Manikandan Panchatcharam, Abdel Salous, Samy Selim, Andrew J.Morris, and Susan S. Smyth
Advances in Hematology, Volume 2012, Article ID 924042, 8 pages
http://www.hindawi.com/journals/ah/2012/924042/
S1P (sphingosine-1-phosphate) is a regulator of endothelial permeability and immune function. Uh-oh, why had I not heard of it? Hmmm…I don’t think it was in Guyton’s or in Harrison’s…and there hasn’t been an RCT about it… Ok, that about explains it.
So here are some factoids about S1P:
– serum levels correlate with HCT as RBCs serve as an S1P reservoir.
– anemic patients’ S1P levels are NOT fully replenished by transfusion, especially the older the transfused blood is.
– In fact, older RBCs may actually remove plasma S1P.
The study:
They basically took mice, and in the first group, bled them (by 20ml/kg) and looked at inflammatory markers, lung permeability and also S1P levels. That’s basically the control group, and they noted that hemorrhage significantly increased inflammatory markers (interesting in and of itself) . They then transfused these mice using wither fresh, S1P-loaded RBCs, or 14-day old RBCs, and, lo and behold, the fresh blood resulted in less inflammation, increased S1P, but most importantly, markedly decreased lung permeability. So clearly, S1P attenuates transfusion associated lung permeability.
In the next group, they injected the mice with LPS following hemorrhage, and found a synergistic effect of blood loss and LPS on inflammation and lung permeability, as could be imagined. Following the LPS, they were transfused with one of four strategies: fresh blood, old blood, fresh blood + S1P or old blood + S1P. Well, lung permeability still increased in all groups, but least in the fresh blood + S1P, and the old blood + S1P a close second.
Note, interestingly enough, that saline alone (the “control”) also increased lung permeability, highlighting yet again that NS (and probably any crystalloid) is not innocuous…
So here we’re looking at the finer effects of transfusion, and why, against “common-sense” correcting a patient’s hemoglobin level does not seem to help in all situations. We have understood the aging issue and loss of deformability, but it is time to take a finer look. We are familiar – at least in concept – with transfusion-associated lung injury or TRALI, but the mechanism remains unclear.
Summary and Take-Home message:
S1P infusions in sepsis? Maybe someday…
Yes, this is an animal study, and the results cannot be extrapolated directly to humans, but it is food for thought, as John had mentioned. Certainly at least this should tell us to keep and ear/eye out for human work with S1P, but personally, it will make me even more comfortable in not transfusing my septic patients with hb’s in the low 70’s and maybe even high 60’s (try repeating the cbc, more often than not comes back a couple points higher and you can avoid transfusion), and for those who are a little more aggressive with transfusion, maybe this should make them think twice…
I’ll add what I can dig up on human S1P studies soon.
cheers!
Philippe
A great surprise this morning: a comment from John. Yup, THE John. So taking a page out of Scott’s book, I thought it would be worth sharing with everyone as its own post, as opposed to just a comment. I think this is must-read material for everyone.
So without any further adue:
“I thought I might add some quirky ideas to your discussion.
We are now getting familiar with the concept of endothelial cells covered by a surface glycocalyx layer, that forms part of the barrier and mechano-sensing functions of the blood-tissue interface. We have discussed in some detail, the role of the glycocalyx in preserving endothelial integrity. I am gonna try and add a bit more spice into the whole transfusion drama.
In recent times, we have started talking a lot about a bioactive phospholipid called sphingosine-1-phosphate (S1P), as a crucial element in preserving vascular barrier integrity by ‘protecting’ the Glycolcalyx. (Most geeky papers on TRALI and other transfusion related complications do mention it).
Because albumin is one of the primary carriers of sphingosine-1-phosphate (S1P), it is possible that S1P, acting via S1P1 receptors, plays the primary role in stabilizing the endothelial glycocalyx. Infact, antagonism of S1P1 receptors have been shown to cause widespread shedding of the glycocalyx, as evidenced by increased serum concentrations of Heparan sulphate and Chondroitin sulphate. (This might probably be one of the mechanisms how albumin is glycocalyx friendly).
RBC transfusions are a double edged sword…..especially in situations of acute anemia as in post hemorrhagic situations ( major GI bleed or trauma.)….I totally agree with you in that the two are conceptually very similar.
Erythrocytes have been identified as an important buffer for sphingosine-1-phosphate . In mice, depletion of plasma S1P by genetic inactivation of S1P synthesizing enzymes (sphingosine kinases 1 and 2) elicits profound pulmonary vascular leak, which can be reversed by restoring circulating S1P via RBC transfusion.
In humans, hematocrit (Hct) predicts plasma S1P levels. There also seems to be a dynamic equlibrium between SIP levels of the plasma, and the circulating RBCs. It has been demonstrated that in anemic individuals, plasma S1P levels are not uniformly restored by RBC transfusion. Rather, the age of the RBC unit at the time of transfusion tended to negatively correlate with the ability of RBC transfusion to replenish plasma S1P. During storage, the S1P content of human RBC markedly declines, likely due to enzymatic degradation. Because erythrocytes serve as a buffer for circulating S1P, aged RBC with low S1P content may be incapable of restoring plasma S1P levels and may actually remove S1P from plasma, which in turn could contribute to increased endothelial permeability, capillary leak, and infiltration of inflammatory cells.
I hope this partly answers your question as to how the glycocalyx may be impacted by inappropriate and irresponsible transfusion triggers. I agree that these are all very novel ideas and as such, exist in the realm of experimental clinical physiology, but my gut tells me that the delicate Glycocalyx may hold the clue to a lot of answers to questions that have plagued us for a long long time!
Cheers,
John from India…”
So first of all, thank you very, very much for reading and taking the time to comment and enlighten us.
As John says, this is still in the realm of experimental physiology, but I think there are a lot of situations we are faced with, perhaps grey zone areas where we debate two potential therapeutic avenues, where we can use some of this data. We might debate giving that extra bit of fluid, or debate crystalloid vs albumin, or blood or no blood with an Hb of exactly 70, and I think we have to start weighing in some of this physiological data, even if it isn’t “evidence-based-by-RTC” to help guide these decisions.
The more I look into it the more it seems that our interventions – particularly fluid resuscitation, needs to be reassessed from the ground up both in nature, quantity and rate of infusion while measuring glycocalyx damage – e.g. biomarkers such as S1P, heparan or chondroitin sulfate, etc…
I’ve previously posted and podcasted about my general strategy for fluid resuscitation, and I am definitely in the process of revising it, still unsure what is best. I’d love to hear how John resuscitates his patients…
thanks!
Philippe
Other Comments:
Mystery John has an uncanny ability to describe complex physiology in the simplest way possible. I am very interested in digging more into his predictions of the possibility of aged erythrocytes removing S1P from circulating plasma.
Dr. John, if you’re out there, could you point us all to some of these studies you’ve mentioned? Any good S1P review papers you’d recommend to those, like me, who are S1P novices?
Thanks for your input! It was a pleasure.
Warm regards,
Derek
Thank you Derek, for the kind comments…. I think the concept of S1P is still in the process of evolving and assuming a definitive shape, so a good review might be hard to stumble across.
A good research article which cites some excellent references might be —
Synergistic Effect of Anemia and Red Blood Cells Transfusion on Inflammation and Lung Injury
— Anping Dong et al. (It is open access at http://dx.doi.org/10.1155/2012/924042).
Hope this helps……
John.
Here is the article:
P
We’re in the final stretch of planning for this year’s conference, which will be totally awesome:
There are a couple of TBA lectures pending confirmation, as well as finalization of the pediatric side, but this should whet your appetites! Final one will be out by the end of the week!
Montreal (awesome spot to visit!) May 9th (pre-congress courses) 10th-11th (main symposium) filled with some really cool clinical lectures on how to integrate ultrasound in common and critical clinical scenarios.
The faculty is awesome:
Andre Denault, Haney Mallemat (@criticalcarenow), Vicki Noble (@nobleultrasound), Mike Stone (@bedsidesono), Edgar Hockmann, JF Lanctot and Maxime Valois (@EGLS_JFandMax), Robert Chen, Catherine Nix, Ashraf Fayad, Michael Woo and many more….
…and lots of intense workshops!
This isn’t just a “how to”, its a “how to really integrate in into daily practice.” or maybe “how to take your game to a whole new level!”
Registration is open, and figure on the final programme to be out by the end of next week.
http://ccusinstitute.org/Symposium6.html
if you have any questions, feel free!
Hope to see you all there!
Philippe
The best is yet to come.
This WordPress.com site is the bee's knees
where everything is up for debate . . .
Brazilian Jiu Jitsu for Wrestlers
Critical discussions on critical care
a blog for thinking docs: blending good evidence, physiology, common sense, and applying it at the bedside!
