
So this morning I shared a case that I’m looking after on Twitter and got asked a really interesting question. But a bit too much for the 140 characters of Twitter. So here’s the answer!
Thanks!
So this morning I shared a case that I’m looking after on Twitter and got asked a really interesting question. But a bit too much for the 140 characters of Twitter. So here’s the answer!
Thanks!
So I ran a couple of twitter polls sets the other day. Here is the first:
(if you want the twitter videos see here)

and part 2:


And to sum it up:

So I just wanted to illustrate something I keep bringing up, essentially that the entire IVC literature based on the AP diameter measurement is physiologically and mathematically flawed. I think the poll and images above clearly support this: given a short axis view, clinicians clearly have a different opinion (and possibly intervention!) than using only a long axis view.
My take, as I’ve said and will keep saying, is that there is a lot of info in IVC POCUS, and the one I am LEAST concerned with is volume responsiveness, which sadly seems to be everyone’s only focus nowadays when it comes to the IVC.
But here’s some food for thought, some of my clinical applications in 5 seconds of scanning:
initial shock patient: big fixed IVC -> no fluids, hurry and find the downstream problem and correct!
resp failure patient: small IVC -> it’s not a massive PE, keep looking for the cause don’t send for a STAT CT angio!
AKI patient: big IVC look at venous doppler and call for lasix, stop the fluids and albumin that were being mistakenly given!
AKI or shock patient & small IVC: sure , start with some fluids and reassess soon (that means hours not the next day)
etc..etc.. there’s more, and “fluid responsiveness” is only in extremes and fairly low on the list for me!
cheers
Philippe
ps if you like physiology, and a physiologico-clinical approach, don’t miss H&R2019!


So sparked by some recent twitter discussions where we were talking about ARDS in a somewhat controversial fashion, I thought it may be worth expanding a bit on the topic.
Essentially my stand is that ARDS is largely an iatrogenic disease mediated by (1) overeager fluid resuscitation of various disease states that fundamentally do not require large amounts of fluids despite commonly held beliefs (sepsis, pancreatitis, etc…) and (2) the absence of frequently used “stop points” of fluid resuscitation with instead a misguided focus on detecting (and intervening upon) volume responsiveness.
In our ICU, true “ARDS” (eg not generated by salt water drowning) is a rarity. Maybe one or two a year, usually a massive primary pulmonary insult.
Anyhow, here, Segun and I discuss this:

Ognjen Gajic refers to this article in our discussion.
So it seems clear that there is much to discuss. We didn’t even really get into the juice of the stop points. Stay tuned!
oh yes… so if these controversial, cutting- and bleeding-edge topics, don’t neglect joining us at H&R2019. Segun and many others will be there!
cheers!


So, venous congestion is the predominant physiopathology in CHF, with a number of ensuing problems including lung edema, effusions, hepatic congestion and cirrhosis, renal failure and even gut edema and failure, though less traditionally focused on.
Venous congestion is essentially a problem of salt and water, retained by a well-intentioned but (eventually) maladaptive neuro-endocrine process. The bottom line being: too much salt and water…
However, the vast emphasis in pharmacologic CHF management, if you look at guidelines and publications, is predominantly on various neuro-endocrine modulation strategies, and though these certainly have a role, it is logical that optimizing volume status must play a central role. So why is it not a recurrent theme of discussion? Well probably because our means to traditionally assess this is limited. What are the tools used by physicians worldwide to assess congestion? Weight, peripheral edema, JVD, crackles, CXR are pretty much it. Now even under the best of circumstances, these are hardly precise tools, and of intermediate specificity. But it is what is available, and taught, and in most cases, does the job fairly well. However, judging by the problem of recurrent admissions for CHF exacerbations, likely not good enough.
The Canadian HF Guidelines – as thorough as they are – are interesting in that the only time diuretics are addressed are in exacerbation, and a note to use the lowest dose possible to maintain stability… But little else in terms of guiding this assessment of stability or the dosage management. The usual “thorough history and physical” stuff, of course.
So what else could we do? Now my interest in POCUS is no secret, and it seems like the ideal tool for assessing both fluid collections and hemodynamics. So what do we know?
Lungs – at this point it’s beyond much debate, POCUS-enhanced physical examination is vastly superior to radiographs and traditional physical examination. Small effusions are easily seen as well as congestion in the form of B lines. In the case of sub-acute to chronic congestion, as we are not overly concerned with central lesions (not seen with ultrasound), the CXR is of no further benefit.
Peripheral edema – I’ll call this one a tie. Not that much benefit in measuring subcutaneous edema with a probe, except for exact reproducibility, at the cost of time. 😉
The Heart – another no-brainer. Ultrasound wins. With appropriate training, experience, and more important than either, the ability to recognize one’s own limitations.
Venous congestion – Now we’re getting to the interesting stuff. So even if for some, it may be the first time hearing about the clinical use of venous congestion markers in CHF, it isn’t new science. In the 90’s, several studies were published correlating portal vein pulsatility, congestion index, as well as hepatic vein doppler pattern with CVP, RV dysfunction, finding close correlation. In 2016, Iida et al published a great article on renal venous doppler and CHF which I highly recommend reading, and more recently, Andre Denault and William Beaubien-Souligny (@WBeaubien) have been doing tremendous work with portal vein pulsatility and post-op cardiac patients’ organ dysfunction. So the science correlating excessive venous congestion to organ dysfunction is there and is clear.
Why have we not yet widely studied this?
The answer is fairly simple. Prior to the growth of POCUS, there was no single clinician group holding the necessary set of clinical and echographic skills to make this clinical routine. Cardiologists are not all echo-capable, and even those that are would have had little or no experience dopplering abdominal organs and vessels. Radiologists – most of the literature coming from their field – are not pharmaco-clinicians and do not follow patients. Family physicians and internists, likely the bulk of the physicians looking after these patients, largely had not had access to or echo skills. Until now.
So a quick review: right-sided failure causes elevated RAP, so everything upstream gets congested. The first echo signal of this is the plethoric IVC (in both axes of course!!!), and an abnormal hepatic vein doppler (which is pretty much like a CVP tracing, just non-invasively) but is that the max? Nope. What is worse is when that pressure transmits thru backwards from hepatic veins to portal vein, transforming a normally monophasic flow with minimal variation into a progressively more pulsatile flow, to the eventual point of being intermittent. And when the IVC pressure transmits across a congested kidney such that the same thing occurs in the renal veins.
Those findings have been well studied and correlate with poor outcomes in CHF.
So what could we do?
What we are doing now is systematically assessing CHF patients in terms of their venous side. What we see so far is that some have full, plethoric IVCs, maybe B lines and effusions, maybe some peripheral edema, but may or may not have those worse markers of abnormal doppler flows, and those who don’t generally don’t have significant organ dysfunction such as renal failure (I discussed this a few years ago in my pre-doppler era in terms of re-thinking common approaches).
So when we find significant portal pulsatility, we diurese aggressively, creatinine notwithstanding. We almost always get an improvement in biochemical markers of renal function within 48-72 hours, with the only really tricky patients being those with severe pulmonary hypertension. More on that in another post.
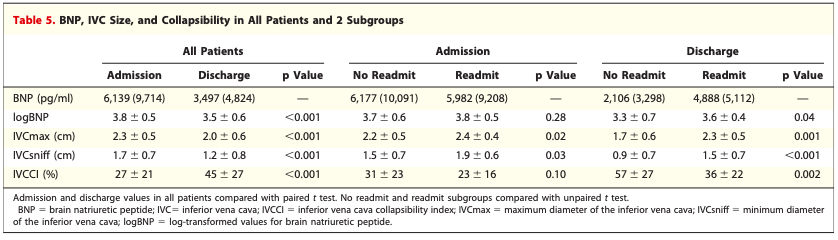
Goonewardena et al had a really great observational study that showed that if CHF patients were discharged with a non-plethoric IVC and significant respiratory variation, they were less likely to be re-admitted. The figure below on the right shows the numbers:
So there is reasonable evidence to suggest a POCUS-guided approach, which we’ll go over in the next post, which should include our revised Advanced CHF Clinic guidelines.
I can already hear the thoughts… “is there any evidence for this?” But those asking that reflexively should first ask themselves “what is the evidence behind the way I assess congestion and manage CHF?”
cheers
Philippe
Refs

(original figure from this old post)
So Rory (@EMnerd) hit us last week with an interesting question that was brought up by David Gordon, a resus fellow working with him, and thought some of us may be willing to belabour his point. A lengthy and really fascinating exchange ensued, which I felt was worth sharing with the #FOAMed community:

Rory (Spiegel @EMnerd) find him on emcrit.org
Korbin Haycock (please leave comments to encourage him to get on Twitter)
Segun (Olusanya @iceman_ex) find him on LITFL.com and The Bottom Line
Me (@ThinkingCC) also thinkingcriticalcare.com
David Gordon
My editorial comments!
Rory:
David brought up an interesting question today. Why not do a straight leg raise and use TAPSE to assess the likelihood the pt will be “volume responsive”?
Lets say we use Korbin’s gold standard I think we still have to ask what is the benefits of giving this pt fluids? There are many patients I see who would meet all the criteria outlined by Korbin in whom I still don’t administer fluids because whatever increase in cardiac output I get will be transient at best. I am inclined to sit tight allow my antibiotics to take effect and let the pt correct their own vasoplegia. After an initial small aliquot of fluid in the ED I like to see obvious signs of hypovolemia before I give additional boluses. I do like the CLASSIC trials criteria:
(1) Lactate of at least 4 mmol/L
(2) MAP below 50 mmHg in spite of the infusion of norepinephrine
(3) Mottling beyond the edge of the kneecap (mottling score greater than 2)
(4) Oliguria
In my mind lactate in and of itself uninterruptible. In a pt who is otherwise improving and the lactate is not clearing as fast as I would like I tend to just stop checking it. The one I find troublesome is in the post resus pt who doesn’t look great, I don’t have an obvious source, their pressor requirements are slowly rising and the lactate is hovering in the 4-5 range. That’s the pt that tends to do poorly if you don’t identify and establish source control
How does the RV respond to a fluid bolus?
To answer this question first we must understand the role of the right heart in the circulatory system. Often the right ventricle (RV) is compared to the left ventricle, in reality it serves an entirely different function. The left ventricle generates the necessary pressures required to maintain systemic perfusion. The right ventricle’s job is to enable venous return, which is generated by the gradient between the mean systemic filling pressure and the right atrial pressure (RAP). The role of the RV is to maximize that gradient by keeping the RAP as low possible.
With this in mind let us examine the RV’s response to a fluid bolus. As the RV becomes filled, conformational changes occur within the RV that allow it to increase its stroke volume without increasing the distending pressure.Under normal circumstances, the RV end diastolic distending pressure does not increase in response to fluid loading. Therefore, if the RV is functioning appropriately, RAP does not accurately reflect RV preload. But in pathological states, when the RV is hypertrophied, diseased, or overdistended there is an inverse relationship between RVEDV and RV stroke volume. Any fluid, or increased RV pressure beyond this point results in an increase in RAP, decreasing venous return.1
1. Pinsky MR. The right ventricle: interaction with the pulmonary circulation. Critical care (London, England). 2016;20:266.
So that was the discussion. I certainly thought it was very interesting. Following this, we decided we’d band together and try to hammer out what we think should be the optimal management of shock, trying to tie in physiology, the scant evidence that is out there about resuscitation, and the pitfalls of venous congestion. Finding the sweet spot in the balance between vasopressors, inotropes and fluids is a very real challenge that all resuscitationists face regularly, and it is very unlikely that, given the complexity of such a protocol, looking at tolerance, responsiveness and perfusion, that an RCT would be done anytime soon.
We’ll be sure to share when we come to a consensus, but certainly the broad strokes can be seen here, and I’d love to hear anyone’s take on this!
And of course, we’ll definitely be discussing this further with smarter people at H&R2019 – think Jon-Emile Kenny (@heart_lung), Andre Denault and Sheldon Magder!
Cheers
Philippe
nice analogy – i think Korbin’s response is appropriate and i look forward to speaking alongside him in May. as i chew on the SHOC-ED a little and try to distill my concerns – i think what it boils down to is this: it’s less about playing with fire – i think – and more about how this fire is brought to the community as a whole. my post on pulmccm was more of a warning to the early adopters [like us] who are planning these trials. imagine 40 years ago:
-the flotation PAC is introduced, a small group of clinical physiologists use it thoughtfully, understand the caveats, the problems of data acquisition, interpretation, implementation, the problems with heart-lung interactions, intra-thoracic pressure, etc.
-these early adopters present their results to the community as a whole
-the physiology of the PAC is simplified
-the numbers from the PAC are introduced into algorithms and protocols and **widely** adopted into clinical practice
-the PAC is studied based on the above and found to make no difference in patient outcome.
-in 2010 a venerable intensivist suggests floating a PAC in a complicated patient and the fellow on rounds chuckles and states that their is ‘no evidence of benefit’
does this sound eerily familiar? is our present rhyming with the past? if the planners of POCUS trials are not careful, i promise you that the same will happen but insert any monitoring tool into the place of PAC. i can very easily visualize a fellow on rounds in the year 2030 scoffing at the idea of PoCUS because trials [SHOC-ED, and future trials x, y and z] showed no difference in patient outcome. is it because PoCUS is unhelpful or is it because the way it was introduced and studied was unhelpful? and the three of us will sound like the defenders of the PAC from 30 years ago: “PoCUS isn’t being used correctly, it’s over-simplified, it works in my hands, etc. etc.”
it’s not PoCUS that’s unhelpful, it’s how we’re implementing it – and i was most depressed when the authors of SHOC-ED appeared to stumble upon this only in the discussion of their paper – like you mentioned phil. imprecise protocols will result in equally imprecise data and the result will be nebulous trial outcomes. we should all be worried.
Korbin adds:
Excellent points Jon. The PAC example is very relevant, as on more than one occasion, I’ve had the argument put to me by some colleagues that essentially how I’m applying POCUS is really no different than the information gleaned from the PAC, and “that’s been shown to not be helpful to outcomes” etc. So, therefore, why do I bother?
Then again, I’ve seen a fair amount of phenylephrine being thrown at hypotensive cardiogenic shock patients after a 2 liter normal saline bolus didn’t do the trick.
You are absolutely spot on when you point out that seeing the big picture, knowing the physiology, and being aware of the pitfalls of isolated data points is important to making the right decisions in patient care.
Furthermore, I agree that when a clinical trial is done that doesn’t consider some of the nuances of all this, and “shows” that POCUS, or any other diagnostic modality for that matter, doesn’t contribute to better patient outcomes, it probably only serves to marginalize a potentially valuable diagnostic tool to an actually astute intelligent clinician.
I’m not meaning by saying this to bash the good intentions of the SHOC-ED trial. To be fair, it’s really hard to design a trial that can take into account all the permutations that are involved in any individual patient presents with, having their own unique clinical situations, hemodynamic profiles, co-morbidities (both known and undiagnosed), etc. POCUS, PAC, transpulmonary thermodilution, ECG, chest x-ray, CT scans, labs, physical exam–these are all merely tools that guide patient care. Albeit some are way more powerful than others. I can image various amounts of uproar if some of these traditional tools were subjected to clinical trials to prove their utility. The argument, if proven “useless” in a study for the oldest and well accepted tools would always be, “put it in the clinical context, and its value speaks for itself.” For me, I’d happily like to make clinical descisions based on information based on an advanced POCUS exam or PAC, rather than interpreting hepatojugular reflux or a supine chest x-ray.
Any diagnostic test requires that the clinician understand the limitations of that test, and understand that the whole clinical scenario must me taken into account. You’ve hit on that, I think, with your argument. This surely has implications when any technology or test is studied.
So this was my comment to my friend Jon’s awesome discussion on the SHOC-ED Trial, which is certainly interesting.
Jon, great post as always! I do agree with most of it, but would have to caution readers about reading it with the filtered glasses that make people too often take home the message that they want to – usually the path of least resistance (or change). I think your main point and most critical one is that there is no protocol or recipe that should ever be applied to resuscitation, especially single-variable-based resuscitation (eg old school orders like CVP>12 lasix and <12 bolus), and substituting the IVC for CVP won’t help. And from a standpoint of volume-responsiveness, I totally agree, with the understanding that as the IVC gets more plethoric, the percentage of responsive patients will decrease, inevitably, but one cannot predict with certainty whether that one patient will or will not. However, the parallel change is that, as the IVC gets more plethoric, the volume tolerance is likely decreasing as well, so that your benefit to risk ratio is dropping. And of course you can’t recipe that just based on IVC, but should be looking at the site of pathology (eg lung, brain abcess, pancreatitis with ACS, etc…), physical exam, to determine your patient’s volume tolerance. Because we all know that most of that miraculous fluid will end up clogging the interstitium, with consequences ranging from cosmetic to fatal (though usually blamed on the patient being “so sick” in the first place, absolving the clinician from any wrongdoing). So comments like the one previous to mine, stating “give volume and see if the response occurs” are, in my mind, a poor approach. We know from studies that you cannot simply remove the fluid you gave and go back to the start with lasix (glycocalyx damage, etc), and we also know that much of the effect of said fluid administration dissipates in minutes to hours (I’m sure Jon can quote these studies off the top of his head!).
As we have discussed in the past, I think POCUS is much underused as a fluid stop point – most of its use is on the ‘let’s find a cool reason to give.’ I would argue that you should hardly ever give fluid to a full IVC (especially if markers of pathological congestion are present – portal vein pulsatility and all), unless you are dealing with temporarily improving tamponade or tension pneumo, because even if you are volume responsive, you are likely not volume tolerant. This also goes to the point that a single, initial POCUS exam will potentially not have the same impact as a whole POCUS-based management which will use it to reassess congestion status, cardiac function, etc.
Having said all this, the most important part of the SHOC-ED article is, in my mind, their discussion, which is full of all the important reasons why the final conclusion is not `we don’t need to do POCUS in shock,’ which is what I see happening (similarly to the TTM reaction), as they outline the cognitive fallacy of putting on trial a diagnostic tool whilst the therapeutics are not yet clearly established. Those only reading the abstract or conclusion will actually miss the important points of this study which the authors clearly explain.
In particular, the ‘rare’ instances of tamponade or aortic aneurysm or PE in their series would be diluted out by the sepsis, but for those patients, it would matter. As the authors state:
‘one might argue that even a single unanticipated emergency procedure would justify the use of POCUS in critically ill patients.‘
I would have to wholeheartedly agree.
cheers
Philippe
This event is past. It was awesome. If you really wish you’d been there, you can catch most of it here!
And don’t miss H&R2020!

Registration is open and we have said goodbye to the snail mail process. Fortunately, we are a lot more cutting edge in medicine than in non-medical technology.
We are really excited about this programme, and a lot of it comes from the energy and passion coming from the faculty, who are all really passionate about every topic we have come up with.
The hidden gem in this conference is the 4 x 40 minutes of meet the faculty time that is open to all. Personally I’ve always felt that I learn so much from the 5 minute discussions with these really awesome thinkers and innovators, so wanted to make it a priority that every participant should get to come up to someone and say ‘hey, I had this case, what would you have done?’ Don’t miss it!
CME Accreditation for 14 hours of Category 1.
This programme has benefitted from an unrestricted educational grant from the following sponsors (listed alphabetically):
Cook
Fisher-Paykel Healthcare
GE Healthcare
Maquet-Gettinge
Masimo
Medquest
MD Management
Medtronic
Novartis
Teleflex
The Accreditation is as follows:

Here is the Final Programme:
Wednesday May 22 – PreCongress course
FOR DETAILS SEE HERE
2. Full day Keynotable
3. Half day Hospitalist POCUS (PM)
4. Half day Critical Care Procedures (AM)
5. Half day Brazilian Jiu-Jitsu for MDs (AM)
for more details on these pre-conference courses please see here.
Main Conference Programme: H&R2019 Full Pamphlet
Social Events:
Thursday May 23rd Meet the Faculty cocktail! 1900 – Location TBA – BOOKMARK THIS PAGE!
FOR ANY QUESTIONS CONTACT HOSPRESUSCONFERENCE@GMAIL.COM.
So we are very, very excited about our pre-conference course lineup. It is simply awesome:
1. Full day Resuscitative TEE (Limited to 20 participants) 0830-1730
H&R2019 REGISTRANTS SHOULD RECEIVE A CODE ENABLING REGISTRATION. FOR ANY QUESTIONS CONTACT HOSPRESUSCONFERENCE@GMAIL.COM.
2. Full day Keynotable 0830-1730
3. Half day Hospitalist POCUS (Limited to 30 participants) afternoon 1330-1730
4. Half day Critical Care Procedures (Limited to 20 participants) morning 0830-1230
5 .Half day Brazilian Jiu-Jitsu for MDs (Limited to 30 participants) morning 0900-1200.
Note that sadly, you have to make some choices. No way to attend it all…
So here is some info to help you make your best pick:

1. Full day Resuscitative TEE: run by none other than Felipe Teran, and featuring Andre Denault as head instructor, this is a unique opportunity for a deep dive into everything about TEE in shock/arrest as well as extensive hands-on training on shock/arrest TEE using state-of-the-art simulators. Participants will obtain an Optional Competency Assessment, providing a Workshop Certificate and a Focused TEE Competency Assessment Checklist certifying completion of 10 proctored examinations.
Limited to 20 participants. 795$USD. Note that conference registrants (minimum one day) will be prioritized for registration to this workshop, with proof of H&R2019 registration required. Remaining spots will be released to non-conference attendees on March 1st, 2019.

2. Full day Keynotable: the brainchild of educator extraordinaire Haney Mallemat, this course is intended for those who want to add some serious game to their presentations and didactic teaching. Sharing tips and pearls that have made him unquestionably one of the best docs to man the stage and podium, this is a rare opportunity not only to leave run-of-the-mill powerpoints behind, but also to enhance your future audience’s learning and become a master presenter.
Registration 495$USD physicians, 375$USD trainees and other health care professionals. Register at http://www.keynotable.net or email info@keynotable.net.
More details here.

3. Half-Day Hospitalist POCUS: Learn absolutely necessary skills for the day-to-day management of your hospitalized patients. It doesn’t matter how good a clinician you are, with ultrasound you will be a better one. Learn from a world-class clinician faculty how to assess the IVC for a number of clinical scenarios, how to assess lungs, do basic cardiac views, diagnose or rule out hydronephrosis, and safely tap ascites or pleural effusions.
Cutting edge today, standard of care tomorrow…
Faculty: Rola, Ajmo, Haycock, Baker, Olusanya
Practice on state-of-the-art simulators, normal volunteers and volunteer patients with true pathology.
Your patients need you to know this.
Limited to 30 participants so that your hands on and faculty experience is maximized. 300$CAN/250$USD

4. Half-Day Critical Care Procedures: If you are not already familiar with these key procedures any resuscitationist should have in their pocket, don’t miss this course. We’ll go over thoracic pigtail insertion, bedside percutaneous tracheostomy and emergency surgical airway, using manikins and natural simulators. Plenty of practice, until you’re comfortable with the techniques. By the end of this activity, participants should be able to independently insert pigtail catheters and perform an emergency surgical airway, and be able to perform a percutaneous tracheostomy with the backup and supervision of an experienced operator.
Faculty: Ajmo, Farkas, Tremblay
Limited to only 20 participants, so don’t wait too long! 300$CAN / 250$USD


5. Brazilian Jiu-Jitsu for MDs: Nope, you didn’t accidentally click on a link. This is part of the pre-conference day. What does it have to do with medicine? A lot. With life? Everything. If you’re already got mad mat skills, come join us for a couple hours of fun. If not, treat yourself to an introduction into a martial art, a sport and even a lifestyle that cultivates physical and mental health like no others. The rest of the conference will change your practice, but this workshop might change your life.
Faculty: Spiegel, Rola, and some guest stars!
No experience necessary, only interest and enthusiasm.
It’s a bit too early to be sure who, but expect to have some interesting surprises as to who your instructors might be…
…oh, and acute care docs should find something in the words of Rickson Gracie, one of the legends of jiu-jitsu:

Limited to 30 participants, registration fee TBA, and will open on november 1st. You can reserve your spot in the meantime by emailing hospresusconference@gmail.com.
So we are really looking forward to these courses. It’s a great opportunity to pick up some important skills and have plenty of time with some awesome instructors, all of whom are hoping to share as much clinical knowledge as possible.
Mark your calendars! Please email hospresusconference@gmail.com with any questions!
The H&R Scientific Committee – St-Arnaud / Zambrana / Rola
So I recorded this for our incoming residents to Santa Cabrini ICU, whom we expect to become well versed in this procedure by the end of their rotation with us. The difference between a smooth and simple insertion – best for both patient and operator, is in the little details.
Figured I might as well put it up on #FOAMed in case anyone else may benefit!
Here is the podcast:
And here is a video displaying the technique.
cheers
Philippe
The best is yet to come.
This WordPress.com site is the bee's knees
where everything is up for debate . . .
Brazilian Jiu Jitsu for Wrestlers
Critical discussions on critical care
a blog for thinking docs: blending good evidence, physiology, common sense, and applying it at the bedside!

So, fresh from reading Jon’s post, I felt I had to add a bit of nuance in my previous post to what I feared some might extract as a take-home message, even if in fact, we are not that differing in opinion at all – which Jon expressed here:
i agree with ultrasound for finding the uncommon causes of shock. these examples seems to permeate twitter and make ultrasound very appealing. because ultrasound is non-invasive, it makes the risk-to-benefit ratio very low for these uncommon but highly-lethal and treatable causes.
but that needs to be compared to the risk-to-benefit ratio of ultrasound for the more common causes of shock – like ‘non-cardiogenic, septic’ etiologies as seen in SHOC-ED. here, “static’ ultrasound [as per the RUSH and ACES protocols] – per SHOC-ED – appears to be neither helpful nor harmful. your read of the discussion is perfect, but i was depressed because it read as if the authors only realized this ex post facto – study of previous monitoring utensils [e.g. PAC] should have pre-warned the authors …
i will take some mild issue with markers of volume responsiveness and tolerance. you are correct on both fronts – but what the data for the IVC reveals – perhaps paradoxically – is that true fluid responders can have a very wide-range of IVC sizes from small to large and unvarying … this was born out in most of the spontaneously breathing IVC papers [airpetian and more recent corl paper] the sensitivity was rather poor.
the same *could* be true for the opposite side of the coin. a large great vein may not mean a volume intolerant patient. i tried to exemplify how that could be so in the illustrative case in my post. an elderly man, with probable pulmonary hypertension and chronic TR who probably “lives” at high right-sided pressures. nevertheless, he likely has recurrent C. diff and is presenting 1. hypovolemic and 2. fluid responsive despite his high right-sided pressures. portal vein pulsatility *could* be quite high in this patient – but he still needed some volume.
the obvious underlying issue here – which I know you are well attuned to – is that a Bayesian approach is imperative. when you PoCUS your patients, you are inherently taking this into consideration – i know that you are a sophisticated sonographer. my hidden thesis of the post is that if ultrasound findings are followed in a clinical vacuum and followed without really understanding the physiology [which can explain clinico-sonographic dissociation – like the patient in my fictitious case]… disappointment awaits.